Download
1 / 60
610 likes | 622 Views
Beyond LDL. Novel Biochemical Markers of Cardiovascular Risk. Why should I care?. Your Patients Know. U.S News and World Report November 25, 2002 Cover Story The Heart Test That Could Save Your Life An easy, new way to help predict your risk of heart attack and stroke.

E N D
Beyond LDL Novel Biochemical Markers of Cardiovascular Risk
Your Patients Know • U.S News and World Report November 25, 2002 Cover Story The Heart Test That Could Save Your Life An easy, new way to help predict your risk of heart attack and stroke
Missing High Risk Patients • 77% of cardiovascular events, • LDL <160 • 46% of cardiovascular events, • LDL <130
Inflammatory hs-CRP, IL-6, IL-18 Fibrinogen sICAM-1 TNF-α, SAA, MPO, sCD40 Oxidized LDL GPX1 activity Nitrotyrosine Homocysteine Cystatin-C Coagulation tPA, PAI-1 Fibrinogen D-dimer Von Willebrand Factor Lipid Markers Lipid Profile Small dense LDL Oxidized LDL LDL Particle No. HDL profiles Lp(a) ApoB/ApoA-1 VAP Natriuretic Peptides BNP N-terminal proBNP ADMA MMP-9 TIMP-1 Potential Markers
56yo female • smoker • untreated HTN (BP 142/85) • TC 220, HDL 35, LDL 125 • Do you treat her?
Framingham Risk Calculating 10yr Risk • 55-59 yrs = 8 pts • TC 200-239 = 4 pts if 50-59 • Smoker = 4 pts if 50-59 • HDL <40 = 2 • SBP 140-159 untreated = 3 pts • TOTAL = 21 pts or 14% 10 yr risk • Recommendations for 10-20% 10-yr risk?
10-20% 10 year risk • Intermediate Risk Moderately High Risk • Pharmacotherapy • LDL>160, maybe 130 • 2004: Option to initiate at 100-129 if more concerning risk factors
What is hs-CRP • CRP—acute phase reactant • hs-CRP—baseline CRP levels (inflammatory predilection) • <1 low risk • 1-3 average risk • >3 high risk • Standardized test nationwide • $62.50
Practice Guidelines • AHA/CDC Scientific Statement January 28, 2003 Measurement of hs-CRP is an independent marker of risk and may be used at the discretion of the physician as part of global coronary risk assessment in adults without known cardiovascular disease. Weight of evidence favors use particularly among those judged at intermediate risk by global risk assessment.
Evidence • Up through 2004 • 19 large scale prospective studies • Independent risk predictor • Better than LDL at predicting CV risk • Predicts risk of metabolic syndrome • Predicts 14 day MI/mortality in CP pts.
Recent hs-CRP Research • Since 2005 • Mixed results • Not independent risk predictor • Increased risk attributable to traditional risk factors that parallel hs-CRP
The Final Answer on hs-CRP • Evidence that lowering hs-CRP decreases cardiovascular events and mortality limited • JUPITER Trial • 15,000 patient RCT • low LDL but high hs-CRP • Statins • Enrollment 2003
Are there effective treatments to lower hs-CRP? • Diet, wt loss, exercise, smoking cessation • Statins • Beta-blockers • ACE inhibitors • Fibrates • Niacin • Rosiglitazone in DM2 • ASA (56% fewer events)
How Could I Incorporate hs-CRP in My Practice? • Moderately High Risk Patients • (10yr Framingham Risk of 10-20%) • Dilemma over whether to treat • Add hs-CRP to lipid profile • hs-CRP >3, high risk • Begin Statin therapy
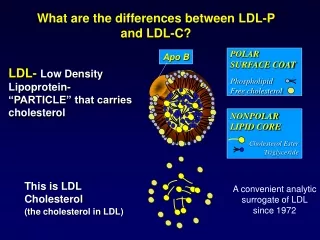
Apolipoprotein B ApoB
Pathophysiology • Apolipoprotein B found on all the atherogenic lipoproteins LDL, IDL, VLDL, Lp(a) • Reflects total # of Atherogenic lipoproteins • ApoA-1 found on HDL • ApoB/ApoA-1 ratio
Evidence • Conflicting results • 175,000 ApoB better than LDL • 12,000 ApoB added no benefit over LDL, HDL, Lp(a), TGs(in women)
Using ApoB to Assess CV Risk • High Risk > 120 • Treatment Target <80 • Statins • Fasting, $70.75
Monitoring Effectiveness of Treatment On Treatment ApoB reflects new risk level
Recommendations • AHA does not recommend testing • Canadian national guidelines have recommended testing since 2001 • March 2006 Journal of Internal Medicine • 10 country panel • ApoB should be included in all guidelines
Lipoprotein (a) Lp(a)
Lipoprotein (a) • Type of LDL bound to ApoB and Apo(a) • Prothrombotic • Binding domain similar to plasminogen, may compete, favoring thrombosis • Proatherogenic • preferentially binds oxidized phospholipids and taken up into atheromatous plaques
Risk Factors • Not associated with most traditional risk factors • Smoking • BMI • Hypertension • Cholesterol subfractions • Exercise and dieting have no effect • Associated with Diabetes mellitus and postmenopausal state
Evidence • Conflicting • PHS, Helsinki Heart and Quebec CV Studies fail to find association between Lp(a) & CV dz • 2 Large Metanalysis show association • Danesh et al. - 27 studies, 10 yrs f/u, combined risk ratio of 1.6 (top 1/3 vs bottom 1/3)
When to Consider? • 1. Premature CV dz w/o risk factors • 2. Strong FH of premature CV dz • 3. Resistent Hyperlipidemia • 4. Hypertension, evidence of early end organ damage
What’s Significant • CMS • Lp(a) > 30 with TChol/HDL > 5.5 • Greater than 90th percentile • 39 in men • 39.5 in women • Higher in blacks
How to Treat? • Unresponsive to statins, bile resin sequestrants, fibric acid derivatives • If high risk based on Lp(a) • Target dropping LDL with statin • If cannot reach target, consider Nicotinic Acid • Omega-3 fatty acids, moderate EtOH, Estrogen
MI 1.7 OR Stroke 2.5 OR PAD 6.8 OR Folate, B12, B6 15 studies 9 studies 5 studies Metanalysis
AHA Recommendation • “[Screening for homocysteine] may be useful in patients with a personal or family history of cardiovascular disease, but in whom the well-established risk factors (smoking, high blood cholesterol, high blood pressure, physical inactivity, obesity and diabetes) don’t exist.”
Hope-2, NEJM April 13, 2006 • Affects of Folic Acid/B6/B12 vs placebo • Homocysteine levels • Outcomes: CV death, MI, stroke • Population: >55yrs with Vascular dz or DM • 5522 pts • 5 year f/u • Over 1000 events
Results • CV death: RR 0.96 (CI 0.81-1.13) • MI: RR 0.98 (CI 0.85-1.14) • Stroke: RR 0.75 (CI 0.59-0.97) • Unstable Angina: RR 1.24 (CI 1.04-1.49)
Conclusion No HOPE for Homocysteine
Evidenced Based Recommendation • Institute for Clinical Systems Improvement: Folic Acid and B vitamins are not recommended for the treatment of hyperhomocysteinemia or the prevention of Coronary Artery Disease (2006)
BNP NT-proBNP
B-type Natriuretic PeptideBNP • CHF • Acute Coronary Syndromes • Risk of Death s/p MI • Prediction of cardiovascular events in asymptomatic individuals
JAMA Apr 6, 2005 • NT-pro BNP, CRP & urinary albumin • Population: older adults (50-89) • Outcomes: mortality and 1st CV events
Significant Details • NT-proBNP only predictor of stroke • 3.63 fold increase risk • Older Adults
Circulation July 5, 2005 • NT-proBNP, CRP, renin • Population: previous stroke or TIA • Outcomes: MI