Download
1 / 24
250 likes | 430 Views
TOS- DISNEA. Dr. Eduardo Gotuzzo Instituto de Medicina Tropical “Alexander von Humboldt” Universidad Peruana Cayetano Heredia. Pneumocystis carinii pneumonia. Between 1981-92 51% had PCP as their initial OI Prophylaxis era: 28% of patients, 1 4.5% as initial OI (NEJM 1993:329:1922-6)

E N D
TOS- DISNEA Dr. Eduardo Gotuzzo Instituto de Medicina Tropical “Alexander von Humboldt” Universidad Peruana Cayetano Heredia
Pneumocystis carinii pneumonia • Between 1981-92 51% had PCP as their initial OI • Prophylaxis era: 28% of patients, 14.5% as initial OI (NEJM 1993:329:1922-6) • Increased risk: CD4 < 200 cells/mm3, oral thrush, prolonged fevers • Mean CD4: 79 (median 36) (Ann Intern Med 1996;124:633-42) • 10% of cases occur with CD4 > 200 cells/mm3 • Symptoms: • Fever • Slowly progressive dyspnea on exertion • Nonproductive cough
PCP in Patients in the Developing Countries • During the first decade of the AIDSpandemic, PCP rarely occurred in African adults • Tuberculosis and bacterial infection were more common • More recent reports have noted that PCP comprises a significantly greaterpercentage of cases of pneumonia than it did in the past • Throughout the developing world, the rate of coinfection with Mycobacteriumtuberculosis and PCP is high, ranging from 25% to 80% Clinical Infectious Diseases 2003; 36:70–8
PCP Diagnosis • Laboratory: LDH in 82-100% • Non specific (disseminated histoplasmosis) • Radiology: • Bilateral symmetric reticular infiltrates • Less Common: Focal or lobar infiltrates, nodules with or without cavitation, pneumatoceles, pneumothorax • Normal Chest X ray in 10% (0-39%) • Sputum • Induced sputum • BAL, TBB
PCP Therapy • High-dose cotrimoxazole (15-20 mg/kg/day of TMP) for 21 days • Second choice: • IV pentamidine, 4 mg/kg per day for 21 days • Alternatives • Clindamycin and Primaquine • Dapsone and Trimethoprim • Atovaquone • Trimetrexate (severe disease requiring IV therapy) • Glucocorticoids if PaO < 70mmHg
HIV & Pneumonia • CAP more frequent than in general population • TB important part of the differential because of high rates of co-infection (30% in Africa) • PCP should be also suspected in newly diagnosed persons and individuals not taking trim/sulfa prophylaxis • CMV pneumonias, Cryptococcus also seen. • Atypical Mycobacteria less common than in industrial countries.
HIV & Pneumonia • Etiologic diagnosis complicated by atypical presentations and limited resources • Empirical therapy encouraged in limited resource settings (CAP vs. TB vs. PCP). • WHO algorithm for managing respiratory tract infection: • Ampicillin or trim/sulfa • TB therapy • 32% cases of pneumonia failed to respond [Mwachari, C. et al JAIDS 2001; 27:365-71] • Infections can present simultaneously (PCP+TB)
HIV & Pneumonia • A significant cause of death in autopsy series (Botswana): TB 45%, bacterial pneumonia 23% [Ansari, N. et al IJTLD 2002;6:55-63] • Respiratory conditions accounted for 14.2% of HIV hospital admissions in Botswana 1997 (TB, bacterial pneumonia) [Steen, T. et al IJTLD 2001; 5:775-82]
HIV & Pneumonia • Almenara Hospital, Lima, Peru (2000): • TB 38/213=17.8% hospitalizations, • CAP & purulent bronchitis, infected bronchiectasis 12/213=5.6% • Pulmonary disease continues to be an important cause of hospitalization in patients receiving HAART: • 9/58 due to respiratory infections (15.5%), • 6 new diagnoses of TB in 45 patients [Almenara Hospital, Lima, Peru, 2003]
HIV & Pneumonia • Bacterial pneumonia is common and occurs with a similar prevalence in HIV-positive and HIV-negative children hospitalized for pneumonia [Zar,H. Et al A Paediatr 2001; 90:119-25]. • HIV-infected children have worse outcome. Case fatality rates and bacterial susceptibility patterns raise the issue of reevaluation of empirical treatment of severe CAP [Zar] [Madhi,S. et al CID 2000;31:170-6]
28 y.o. female, diagnosis of HIV in 10/01. Admitted for 1 month cough, fever, weight loss. Sputum for AFB: positive. Current CD4 350.
32 y.o. female, known HIV since 1999, past history of TB and PCP, developed bronchiectasis. Multiple admissions for purulent bronchitis. Chronic respiratory insufficiency. Intolerance to multiple HAART regimens. CD4 18
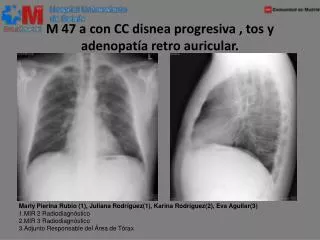
CXR of a 26 yo patient with AIDS with proven Cryptococcus infection depicts extensive right hilar and mediastinal adenopathy and presence of parahilar airspace consolidation. CD4 41.
HIV-positive 25 y.o. male, originally from Pucallpa. 6 month-history of fever and weight loss, chronic cough, occasional hemoptysis and left sided chest pain. Bronchoscopy positive for both Histoplasma and M. tuberculosis
Métodos • Estudio observacional, prospectivo. • Criterios de inclusión: - Pacientes VIH/SIDA con síntomas respiratorios por 7 días o más o insuficiencia respiratoria. - Consentimiento informado • Criterios de exclusión: - Diagnóstico clínico de infección respiratoria alta - Pacientes en tratamiento por episodio actual de enfermedad respiratoria • Aprobado por el Comité Institucional de Etica (UPCH)
Firma de consentimiento Informado Llenado de ficha clínico-epidemiológica Educación y entrega de frasco para muestra 01 de esputo Paciente es evaluado por Enfermera del estudio y cumple criterios de inclusión /exclusión PRIMER DIA
Recolección de 3 ml de esputo SEGUNDO DIA Toma de muestra de sangre: 5cc BACTERIOLOGIA : -Cultivo en LJ -BK directo -Concentración HSSH -Gram. 3CC INMUNOLOGIA -CD4 -Otros 1CC: MICOLOGIA -Serología 1CC: SEROTECA -Backup Llevar 2 láminas extendidas a Micología: -Giemsa -O Toluidina Toma de placa de Tórax
TERCER DIA Recolección de 3 ml de esputo • MICOLOGIA: • -Cultivo para hongos • -Inmunofluorescencia P.carinii • -Giemsa 2 • -O Toluidina • KOH • Tinta China Enviar el sobrante de muestra a Lab. Microbiologia: -BK directo
Rutina de seguimiento • Fecha de inclusión: DIA 0º • 1º Control : DIA 3º • 2º Control : DIA 7º • 3º Control : DIA 14 • 4º Control : DIA 28º • 5º Control : DIA 60º • 6º Control : DIA 90º
Resultados preliminares • Del 22 de Agosto del 2003 al 15 de Mayo del 2004. • Número de pacientes incluidos : 165 • Número de pacientes excluidos: 53
Recuento CD al ingreso Recuento CD al ingreso Percentiles 1% 1 25% 15 Observaciones: 163 50% 49 Media: 111.98 DE: 156.55 75% 159 90% 284 95% 411 99% 854
DIAGNOSTICOS Diagnosticos • PCP : 86 (52.1%) • Sin Dx. Definitivo : 25 (15.2%) • TBC : 22 (13.3%) • Bronquitis : 18 (10.9%) • PCP Y TBC : 6 (3.6%) • Otros : 8 (4.8%) TOTAL 165
CausasCausas de fallecimiento* Causas de fallecimiento* • Insuficiencia respiratoria : 8 • SIDA terminal : 7 • Hipertensión endocraneana : 1 • Anemia Aguda : 1 • Falla multiorgánica : 2 • TBC Multisistémica : 1 • Pendiente revisión de historias : 8 Total : 28 * Como se registra en la epicrisis
Impacto de TBC y PCP en la mortalidad • Fallecidos con PCP : 10 (35.7%) • Fallecidos con TBC y PCP: 5 (17.8%) • Fallecidos con TBC: 7 (25.0%) • Fallecidos sin PCP/TBC: 6 (21.4%) TOTAL FALLECIDOS 28