Download
1 / 32
340 likes | 898 Views
Measles, Mumps, Rubella, Varicella. MedCh 401 Lecture 6. Measles, Mumps, Rubella. Common childhood diseases May be associated with severe complications/death More often in adults Measles - pneumonia, encephalitis Mumps - aseptic meningitis, deafness, orchitis

E N D
Measles, Mumps, Rubella, Varicella MedCh 401 Lecture 6 KL Vadheim Lecture 6
Measles, Mumps, Rubella • Common childhood diseases • May be associated with severe complications/death • More often in adults • Measles - pneumonia, encephalitis • Mumps - aseptic meningitis, deafness, orchitis • Rubella - congenital rubella syndrome • Respiratory transmission KL Vadheim Lecture 6
Measles • 14-day incubation period for respiratory-acquired infections • 6-10 days if acquired parenterally • remains the leading cause of vaccine-preventable death in children KL Vadheim Lecture 6
Measles virus attenuation • Start with attenuated Enders’attenuated Edmonston strain • Propagate in chick embryo cell culture KL Vadheim Lecture 6
Measles vaccine efficacy • 1941 - 894,134 U.S. cases • 1995 - 288 U.S. cases KL Vadheim Lecture 6
Vaccine failure • Infants vaccinated at <12m who were born to naturally-infected mothers may not develop sustained antibody levels when later revaccinated • Primary failure • No seroconversion • Secondary failure • Loss of protection after seroconversion KL Vadheim Lecture 6
Mumps Pathogenesis • Viremia common, leading to organ involvement • salivary glands (parotitis), meningitis, orchitis, endolymph infection leading to deafness • A major cause of permanent, bilateral, sensorineural deafness in children • Virus shed in saliva and urine for long periods after infection KL Vadheim Lecture 6
Mumps Pathogenesis • Reinfection occurs • usually asymptomatic KL Vadheim Lecture 6
Mumps virus attenuation • Jeryl Lynn (B level) strain • Cultured from Jeryl Lynn Hilleman’s throat • Attenuated by serial passage in • embryonated hen’s eggs • chick embryo cell culture KL Vadheim Lecture 6
Passive immunization against mumps • Immune globulin ineffective for postexposure prophylaxis • does not prevent disease or reduce complications • Transplacental maternal antibody appears to protect infants for first year of life KL Vadheim Lecture 6
Mumps vaccine efficacy • 1968 - 152,209 U.S. cases • 1995 - 840 U.S. cases KL Vadheim Lecture 6
Recent mumps outbreaks • Started in Dec. 2005 in Iowa • 2,597 cases Jan. 1- May 2, 2006 • 11 states, all ages affected • Vaccination clinics initiated KL Vadheim Lecture 6
Theories on outbreak • College campuses are the perfect environment for spreading a disease transmitted through oral secretions • Only 25 states and DC require two doses of MMR for college admission KL Vadheim Lecture 6
More theories • Delayed recognition and diagnosis of disease: • few younger MDs have seen the disease • Many would not consider the diagnosis in a vaccinated individual KL Vadheim Lecture 6
UK Mumps epidemic, 2004-2005 • >70,000 cases in England and Wales • Increased susceptibility of unvaccinated cohorts who have less exposure to mumps because of a decrease in disease circulation after implementation of a childhood immunization program KL Vadheim Lecture 6
UK Epidemic • Importance of ensuring high levels of immunity among other age groups when mumps vaccination is added to the routine immunization schedule for children. KL Vadheim Lecture 6
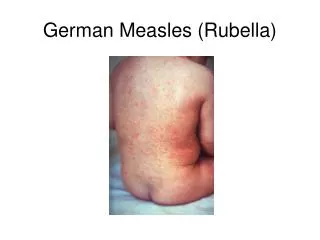
Rubella • Aka ‘German’ measles • Discovered in 1841 • Virus isolated in 1941 by German scientists • Sudden pandemic in 1962-65 • Vaccine developed in 1960s • Vaccine licensed in 1970 (U.S.) KL Vadheim Lecture 6
Congenital Rubella Syndrome • Infection in first trimester most dangerous • 90% of fetuses likely to have some type of abnormality • Virus disrupts organogenesis • plus more destructive on brain, cochlea, lens, etc. • Virus establishes chronic infection in many cells/organs • virus secretion may persist for years KL Vadheim Lecture 6
Congenital Rubella Syndrome • Cataracts • Deafness • Heart malformation • Also: • microcephaly • autism • mental retardation • Diabetes • etc. KL Vadheim Lecture 6
Mumps Pandemic 1962-65, Europe and U.S. • 12.5 million mumps cases • 20,000 cases CRS • 11,600 deaf • 3,580 blind • 1,800 mental retardation • 6,250 spontaneous abortions • 5,000 surgical abortions • 2,100 stillborn/neonatal deaths KL Vadheim Lecture 6
Rubella vaccine • Mumps virus RA-27/3 isolated from an infected fetus in 1965 • Culture fluid passaged directly into WI-38 cells • 8 serial passages at 37C • Seven additional passages at 30C • human volunteer studies showed attenuation • Ten additional passages to further decrease pathogenicity KL Vadheim Lecture 6
Rubella RA27/3 vaccine strain • Produced between 25th and 30th passage in human diploid cells • Relatively rapid attenuation due to: • cold adaptation (30C) • Retention of high immunogenicity due to: • relatively low passage number required for attenuation KL Vadheim Lecture 6
Rubella points to remember • Clinical rubella has been demostrated in vaccinees and naturally infected, immune persons • Reinfection with fetal transmission of wild virus in presence of both natural and vaccine-induced immunity • can result in CRS KL Vadheim Lecture 6
Rubella vaccine efficacy • 1969 - 57,686 U.S. cases • 1995 - 200 U.S. cases KL Vadheim Lecture 6
MMR Vaccines • Live • Attenuated • Subcutaneous administration • Lyophilized presentation • Licensed 1971 KL Vadheim Lecture 6
MMR Vaccines KL Vadheim Lecture 6
Varicella zoster • Causes two separate diseases • chickenpox (varicella) • shingles (herpes zoster) • Generally a benign, self-limiting disease • Herpes virus • Highly communicable disease of all ages KL Vadheim Lecture 6
Varicella Transmission • Airborne • Skin, Respiratory droplets through conjunctivae or mucosa of upper respiratory tract • Can transmit chickenpox to a susceptible person from a person with shingles KL Vadheim Lecture 6
Varicella Pathogenicity • Usually a mild disease • can cause severe, life-threatening complications • 1st trimester infection can cause permanent CNS (and other) damage to fetus, or death • 3rd trimester infectionmay cause severe maternal infection, • Host range limited to humans and some primates KL Vadheim Lecture 6
Varicella Pathogenicity • Latent infection of sensory nerve ganglia common • Some viral infection during latent stage • Suppression of VZV reactivation partially under immunological control KL Vadheim Lecture 6
Varicella Vaccine • Lyophilized • Requires storage at +5F or below • Live, attenuated virus KL Vadheim Lecture 6
Varicella attenuation process • Initial viral isolation from a child with varicella • Adapted to human embryonic lung cell cultures • Adapted to and propagated in embryonic guinea pig cell cultures • Propagated in human diploid cell cultures (WI-38) • Further passage in human diploid cell cultures (MRC-5) that are free of adventitious agents KL Vadheim Lecture 6