Download
1 / 35
360 likes | 509 Views
Infectious Diseases: Investigation, Surveillance, & Prevention. Communicable Disease Section County of San Bernardino Department of Public Health Stacey A. Davis, MPH Epidemiologist. San bernardino department of public health. COUNTY OF SAN BERNARDINO DEPARTMENT OF PUBLIC HEALTH

E N D
Infectious Diseases: Investigation, Surveillance, & Prevention Communicable Disease Section County of San Bernardino Department of Public Health Stacey A. Davis, MPH Epidemiologist
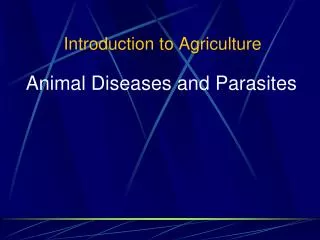
COUNTY OF SAN BERNARDINO DEPARTMENT OF PUBLIC HEALTH COMMUNICABLE DISEASE SECTION ORGANIZATION CHART, POSITION NUMBERS FY 2011-2012 Program Manager Vanessa Long TB Controller Louise McNitt, MD Secretary I Joyce Hall PH Program Coordinator Lea Morgan PH Clinic Supervisor Jenny Hernandez Epidemiologist Stacey Davis HES I Pooneh Navab Faith Mwiti Supervising HSA Leticia Navarette RN II Terri Serna Olu Teiko LVN II Jennifer Rosales HSA Suzie Martinez Katherine Myers Bac Lam Rigo Fernandez Denise Ramirez CDIs Vicki Williams Roger Gonzalez Anita Haro-Garcia Celia Saucedo-Smith Denise Leon HSA Mayra Parga Beverly Villa OA II Maricela Hernandez Diane Hardy
Title 17, section 2500 California Code of Regulations (CCR) • Requires physicians and laboratories to report: • >85 communicable diseases • Any occurrence of unusual disease • Any outbreak • Non-communicable conditions • Animal bites (also for rabies exposure) • Disorders characterized by lapses of consciousness • Alzheimer’s disease and other dementia • Specifies reporting timelines • Allows for the local Health Officer to add any conditions for local reporting
SummarySBDPH Communicable Disease Section • Investigation: individual cases & outbreaks • Surveillance: • Passive for all diseases except TB contacts • Active for identifying TB contacts (potential cases) • Prevention: • Case-patient education re: disease transmission & vaccination, • TB screening for contacts to active TB case • Provider education on vaccine administration for vaccine-preventable diseases • Information resource http://www.sbcounty.gov/pubhlth/ 1.800.722.4794
Norovirus • Etiology: group of related non-enveloped RNA virus • 5 genogroups, 3 important in humans (GI, GII, GIV) • >25 different genotypes identified within these genogroups • Symptoms: watery non-bloody diarrhea, nausea, vomiting, abdominal cramps, low-grade fever • In children, diarrhea more common that vomiting • Studies have shown asymptomatic infection can occur in as many as 30% of infections
Norovirus • Incubation period: 12-48 hours (commonly 24-48h) • Infectious period:Few hours before onset to 72 hours after symptom resolution • Transmission: fecal-oral
Viral Gastroenteritis (VGE) Outbreak Investigation • Identify: What is above baseline? Suspect etiology? • Notify: • Licensing & Certification • County of San Bernardino Dept. of Public Health • Linelist: Collect case information • Name • Age • Location in facility (room, wing, unit, etc.) • Symptoms, including hospitalizations • Specimens collected & results • Establish case definition (work with DPH) • Implement prevention & control measures
Norovirus: Prevention & Control CDPH Recommeds: Residents • Cohort, if possible • Restrict movement: new admissions, transfers • Cancel group activities, dining • Clean equipment & facility surfaces* • Education Staff • Cohort, if possible • Restrict ill staff, visitors, volunteers from work • Use PPE for symptomatic residents, cleaning • Education
Important Contributory Factors to Outbreak Spread • Environmental persistence • Withstands freezing and temps up to 140 degrees F • Check your ice machine! • (**how lon • Short incubation period • High Infectivity • Low infectious dose: 10-100 viral particles is sufficient to cause infection • Viral shedding can begin before symptom onset • Viral shedding can occur up to 2 weeks after symptoms stop, but it is unclear how viral shedding after 72h post-recovery contributes to infectivity • Immunity is short-lived (a few months) and strain-specific
Norovirus Resources • County of San Bernardino Dept Public Health, Communicable Disease Section • Linelist template (MS Excel) • Norovirus checklist • Handwashing signs (electrostatic) • Laboratory testing for Norovirus (min 2, max 4 specimens) CDPH • Recommendations for the Prevention & Control of Viral Gastroenteritis Outbreaks in California Long-Term Care Facilities , October 2006 • Acute Viral Gastroenteritis Investigations in Residential Facilities http://www.cdph.ca.gov/pubsforms/Guidelines/Pages/HAIandIC.aspx • CDC Norovirus page http://www.cdc.gov/ncidod/dvrd/revb/gastro/norovirus.htm
Scabies • Etiology: human itch mite, Sarcoptesscabieivarhominus • Symptoms: • Intense itching; • Papules, vesicles, tiny linear markings containing mites & eggs, mainly around finger webs, groin, anterior wrists, elbows, other skin folds • Possible secondary skin infections from itching • Crusted lesions (immunecompromised or elderly patients) • Few with immunecompromised patients or patients with neurological conditions
Scabies • Incubation period: • 2-6 weeks (without previous exposure); • 1-4 days (with previous exposure) • Infectious period: time of infestation (even if sx absent) to completion of at least 1 treatment with scabicide • 2 treatments for highly infested individuals, 1 week apart • Transmission: • direct skin contact with infected person, including sexual contact • Shared fomites (clothing, bedding)
Scabies Outbreak Investigation • Identify: skin scrapings • Symptomatic case, resident, or healthcare worker • Outbreak: 2 or more confirmed cases OR 1 confirmed case and 2 suspect cases during a 2 week period • Notify: • Licensing & Certification • County of San Bernardino Dept. of Public Health
Scabies Outbreak Investigation • Linelist: collect case and contact information (during 4 weeks before case’s onset) • Name • Age • Location in facility (room, wing, unit, etc.) • Symptoms, including hospitalizations • Specimens collected & results • Transfers to other facilities
Scabies Outbreak Prevention & Control • Isolate cases • Use PPE to apply scabicide to cases • Bathe case before application (if not bathed >24h) • Bathe case after 8-12h treatment to remove scabicide • Restrict visitors (or ask to use PPE) • Launder all washable items in hot soap & water, dry on high • Separate from all other laundry • Bag all non-washable items for 7 days • Disinfect equipment, mattresses, etc. after scabicide washed off • Discard any topical creams, ointments, lotions used by symptomatic cases
Scabies Outbreak Prevention & Control—Atypical Scabies Atypical Scabies • Isolate case in private room until at least 2 treatments and 2 negative skin scrapings • Remove upholstered furniture from room & cover with plastic for 7-10 days Crusted or Norwegian Scabies • Isolate case in private room until at least 3 negative skin scrapings, may take 7-30 days or longer • Remove upholstered furniture from room & cover with plastic for 7-10 days
Scabies Prevention & Control: Contacts • Evaluate contact • Can contact be substantiated? • What type of contact? Direct or indirect? • If substantial contact, treat both asymptomatic & symptomatic contacts 1X • Treat all contacts and cases during the same treatment period • Allow to return to work after one 8-12h treatment • Allow non-contacts one treatment, if requested
Scabies Treatment Failure • Poor application technique • Apply from hair & ear line to palms & soles of feet • Continued contact with untreated or unsuccessfully treated residents, HCWs • Reluctance of HCW to disclose sx • Residents, staff with immunosuppressive diseases who don’t respond to treatment • Use of topical steroids during treatment period • Failure to kill mites in clothing, furniture
Scabies Resources • County of San Bernardino Dept Public Health Communicable Disease Section • Linelist template (MS Excel) • CDPH Scabies Prevention & Control Guidelines • Outbreak management CDPH • Healthcare Associated Infections & Infection Control Guidelines page http://www.cdph.ca.gov/pubsforms/Guidelines/Pages/HAIandIC.aspx • CDC Scabies page http://www.cdc.gov/parasites/scabies/
Influenza • Etiology: influenza virus, types A, B • Symptoms: Fever, cough, sore throat, runny or stuffy nose, muscle or body aches, headaches, fatigue • Incubation period: 2 days (range 1-4 days) • Infectious period: highest 3-5 days after onset, up to 7-10 days • Transmission: droplet and contact spread
Influenza Outbreak Investigation • Identify: • Acute onset of fever and cough; • LTCF residents not always typical presentation • Laboratory testing recommended • Cluster: 3 or more cases of acute respiratory illness within 48-72h in residents in close proximity • Outbreak: sudden increase in acute respiratory illness over background rate OR one positive test for influenza in a resident
Influenza Outbreak Investigation • Notify: • Licensing & Certification • County of San Bernardino Department of Public Health • Linelist (both Staff & Residents) • Name • Age • Location in facility (room, wing, unit, etc.) • Symptoms, including hospitalizations • Specimens collected & results
Influenza Prevention &Control • Isolate symptomatic resident & exposed roommate(s) in room • Cancel group activities & dining • If many residents ill • Serve meals in rooms • Cohort residents & staff, if possible • Limit new admissions • If necessary, admit to unaffected units • Use PPE—Residents • Patient use surgical mask if transported
Influenza Prevention & Control • Use PPE—Staff • Staff use surgical mask, gloves, gown when within 3 ft of patient or entering resident’s room & contact anticipated • Remove after leaving room, dispose in waste receptacle • Wash hands after PPE removal • Provide many waste receptacles • Encourage hand washing • Exclude ill staff from patient care for 5 d after onset of sx • Encourage not to work in other facilities (both ill & well staff)
Influenza Prevention & Control • Enhance environmental cleaning of surfaces • Treatment & prophylaxis: CDC Recommends • Do not useamantadine or rimantadine(amantadines) • (increased resistance in Influenza A viruses) • Do useoseltamivir (Tamiflu) & zanamivir (Relenza) • Treat within 2 days of onset • May still be beneficial if after 2 days of onset in patients with severe, complicated, or progressive illness • Treat confirmed and suspected cases (do not wait for lab confirmation)
Influenza Prevention &Control • CDC recommends vaccinating staff & residents • Every year • After outbreak identified, if unvaccinated • Standing orders for residents >50yo for pneumococcal vaccination & annual influenza vaccination • Declination form for staff & residents • Vaccination pledge (optional)
Influenza Resources • County of San Bernardino Dept Public Health, Communicable Disease Section • Linelist template (MS Excel) • CDPH Recommendations for Prevention & Control of Influenza in LTCF • Outbreak/cluster management • CDPH • Healthcare Associated Infections & Infection Control Guidelines page http://www.cdph.ca.gov/pubsforms/Guidelines/Pages/HAIandIC.aspx • CDC 2011-2012 Influenza Antiviral Medications Recommendations • http://www.cdc.gov/flu/professionals/antivirals/summary-clinicians.htm
Pertussis (Whooping Cough) • Etiology: Bordatellapertussis(bacteria) • Symptoms: Cold-like symptoms, cough that progresses to become paroxysmal and last up to 2 mo, sometimes post-tussive vomiting • Incubation period: 6-20 days (9-10 days avg) • Infectious period: 21 days after sx onset, or 5 days after start of appropriate antibiotics • Transmission: Airborne via droplets • Public Health Significance: • Can be lethal in children <6mo • Pregnant women • Contacts to children <6mo
Pertussis (Whooping Cough) • Identify: • Testing (PCR or culture) • Symptoms • Notify: • Licensing & Certification • County of San Bernardino Department of Public Health • Linelist (both cases and contacts) • Name • Age • Location in facility (room, wing, unit, etc.) • Symptoms, including hospitalizations • Specimens collected & results • Vaccination status
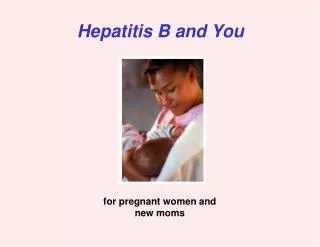
Pertussis (Whooping Cough) • Implement prevention & control measures • Exclude case/limit contact while infectious • 5 days after appropriate treatment completed OR • 21 days after cough onset • Antibiotic prophylaxis to close contacts & high risk contacts • Pre-exposure: Vaccination with Tdap Antibiotics given End if antibiotics given Onset of sx Infected END Infectious Period Exposure 5 -10 0 10 …21
Pertussis outbreak in California • 9,477 cases for 2010 has surpassed the number of cases reported in 1947 • State rate of 24.2 cases/100,000
Pertussis Resources • County of San Bernardino Dept Public Health, Communicable Disease Section • Linelist template (MS Excel) • CDPH PertussisQuicksheet • Outbreak/cluster management • CDPH • Pertussis (Whooping cough) page http://www.cdph.ca.gov/HealthInfo/discond/Pages/Pertussis.aspx • CDC Pertussis page • http://www.cdc.gov/pertussis/
Questions? Thank you!



![EVM System Surveillance Presented By: [NAMES] Presented to: [GROUP]](https://cdn0.slideserve.com/294105/slide1-dt.jpg)