Download
1 / 34
340 likes | 496 Views
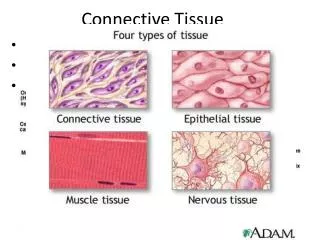
Connective tissue. Bone. Karel Šulc. Connective tissue. functions : cell growth, cell differentiation, cell communication with

E N D
Connective tissue. Bone Karel Šulc
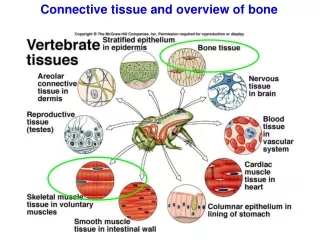
Connective tissue • functions: cell growth, cell differentiation, cell communication with • extracellular matrix retention of water (maintenance of tissue turgor) retention of minerals in the bone „store“ of many cytokines controlling cell proliferation • disturbances of the connective tissue disturbances of morphogenesis, creation of the tumor metastases, disturbances of wound healing • composition of extracellular matrix fibrous structural proteins (collagen, elastin) adhesive glycoproteins (fibronectin, laminin) gel (proteoglycans, salts of hyaluronid acid) • these macromolecules co-creates basal membranes (products of epithelium + mesenchymal cells) composition: non-fibrillar collagen (IV), laminin, proteoglycans
Cells of connective tissue. Matrix • fibroblasts standing production of collagen, amorphous matrix in some tisues chondrocytes, osteoblasts-osteocytes, synoviocytes • macrophages (antigen present cells) participation in immune reactions, synthesis and release of the cytokines, phagocytosis • mast cells, lymphocytes, plasmacells immune response • reticular cells synthesis of the reticular fibres; phagocytosis • matrix free suspension of petides and proteins, lipids, mucoproteins, glycoproteins, mucopolysacharides acid mucopolysacharides (glycoseaminoglycans) bound of water
Connective fibres • collagen triple helix of polypeptide chains α1, α2, α3 • α-chains synthesis in ribosomes postribosomal processing hydroxylation of proline and lysine remnants; thus high amount of hydroxyproline and hydroxylysine in the moleculevitamin C is need to the hydroxylation (it is also need to wound healing) • after hydroxylation of the chains, triple helix is created; fibrills are created due to influence of pro-collagene peptidase; rise of the collagen is qualified by rising of cross-linked bounds among chains • defect both in synthesis and structure of the collagene Ehlers-Danlossyndrome
Connective fibres • elastic fibres (elastin, fibrillin)importance in function of some tissues (vessels, lung, derma, uterus etc.) • stretching force collagen fibres, original size of tissue is realized by elastic fibres) • fibroblasts + myocytes production of elastic fibrescontent: great amount of proline, lysine, no hydroxyproline, hydroxylyzine • composition: core(elastin, mw. 70kD) surrounded with net of microfibrils(glycoproteinfibrillin, mw. 350 kD) • mutation of fibrillin gene synthesis of abnormal elastic fibresMarfan syndrome
Influence of some hormons in connective tissue • glucocorticoidsinhibition of the acid mucoprotein synthesis disturbance of collagene fibres and matrix synthesis (proteocatabolism) (Cushing syndrome, overdose of the glucocorticoids enhanced vessel fragility, loss of derma elasticity, prolonged wound healing • hypothyroidismhigh content of mucopolysacharides and hyaluronic acid (bound of water) in subcutaneous tissue (myxoedema) • hyperthyroidismdecrease in amount of acidmucopolysacharides • GH stimulation of the connective tissue, thickening of derma and subcutaneous tissue, creation of hypertrophic scars • estrogenes synthesis of mucopolysacharides is stimulated • progesterone inhibition of MPS synthesis
disturbances of the connective tissueresponse to injury wound healing and its disturbancereaction of connective tissue is affected by nutritionendocrine system function agingdeficiency of the proteinsdeceleration of wound healing, restriction of the connective tissue resistivity against tensile loadingdeficiency of ascorbic acid disturbance of collagene fibre function due tolack of hydroxyproline and hydroxylysine in collagene chains
Diseases of the connective tissue • evoked by inflammatory processdegenerative state • primary inflammation degenerative process • system of locomotion is primarily involved • synovitis (inflammation of the articular cavity) acute form exudative inflammation fluid retention in the capsule + great amount of PMNCdilation of vesselsacute form chronic form (proliferation phase)
Marfan syndrome • disorder of the connective tissue, manifested principally by changes in the skeleton, eyes, cardiovascular system • pathogenesis inherited defect in an extracellular glycoprotein – fibrillin. It is major component of microfibrils found in the extracellular matrix in organism, abundant in aorta, ligaments, ciliary zonules of the lens • genes FBN1 and FBN2 encode fibrillin1 and fibrillin2mutation of FBN1 – Marfan syndrom, mutation of FBN2 – inherited arachnodactylia. Mutant fibrillin1 disrupts the assembly of normal microfibrills. • skeletal abnormalities: patient is unusualy tall with exceptionally long extremities and fingers, the joint ligaments are extremelly lax (e.g. thumb can be hyperextended back to the wrist). Variety of spinal deformities (kyphosis, scoliosis) • eye – bilateral subluxation or dislocation of the lens (ectopia lentis) • cardiovascular system – life-threatening complications: progressive dilation of aortal valve ring, dilation of the ascending aorta due to medionecrosis, intramural hematoma (aneurysma dissecans) in 30 – 40% cause of death (rupture of ao. wall)
Ehlers-Danlos syndroms • genetically and clinically heterogeneous group of disordersbase: defect in synthesis and structure of collagene • tissues rich in collagene are frequently involved – skin, ligaments, joints • skin is hyperextensible and fragile, joints are hypermobile • the basic defect in collagen synthesis and structure may lead to serious internal complications: rupture of the colon and large arteries, ocular fragility with rupture of cornea, diaphragmatic hernias • biochemical and molecular base is known only in few forms of EDS – e.g. mutation of the gene encoding lysyl-hydroxylase (hydroxylysine is necessary for crossing of the collagen fibrills) synthesis of the collagen with disturbed structural stability
Lupus erythematosus • multiorgan disorder – joints, skin, lungs, kidneys, CNS • onset 20 – 30, acute state, later chronic state♀ 9 : ♂1 • etiology – unknowngenetic predisposition + sex hormone influenceUV radiation, D-penicillamin, hydralazine, procainamidviral infection – EBV, cytomegaloviruses • pathogenesis – autoantibodies against nuclear antigenes (DNA, RNA, histones, non-histone proteins bounded to RNA
Lupus erythematosus • joints – non-erosive synovitis • skin – cell destruction in stratum basale, oedema in dermis, vasculitis, vascular necrosis • kidneys – various forms of glomerulonephritis (deposition of complexes DNA-antiDNA, RNA-antiRNA in basal membranes of glomeruli) • cardiovascular system – pericarditis, endocarditis, atherosclerosis • lungs – bronchitis, pleuritis • area v. portae – vasculitis • CNS – vasculitis, focal neurologic signs
Osteoarthritis • chronic disorder without systemic component • characterization progressive erosion of articular cartilage focal loss of cartilage, following hypertrophy of the adjacent bone and cartilage (creation of osteophytes) • joints of upper and lower limbs are involved (knee-hand disease) • etiology:trauma – common cause of monoarticular disorderaging – age related changes in cartilage include alteration in proteoglycans and collageneobesity – metabolic changes in cartilage in the course of obesity are hallmarkgenetic factors – polygenic typ of heredity
Osteoarthritis • disturbance of the articular cartilage – thickness (water, extracelular matrix) • chondrocyte proliferation – reparation is evident • consequently attenuation of hyaline cartilage • enhanced bone remodeling and bone hypertrophy (main sign of OA) – destruction of the bone surface • enhanced proliferation of osteoblastsnew formation of the bone is not in concordance with neoangiogenesis source of bone necrosis • osteophytes disturbance of the joint surface and articular motion • Clinically: articular pain, progressive loss of function
Osteoarthrosis • heterogenous group of diseases – morphological base in all is uniform • multifactorial disease etiology: genetic predispositionagingmechanical influences – joint geometry, capsule flowing endocrine factors – diabetes mellitus, acromegalyimmune disturbaces – deposition of immunocomplexes in cartilages, autoantibody creation • proces is started by biochemical changes in cartilages – loss of proteoglycans; in chondrocytes change in colagene synthesis • loss of cartilage resistivity; bone sclerotization, cysts, osteophytes • clinically: articular pain (free nerve endings in synovia, in periosteum are stimulated) (cartilage does not content nociceptors), progressive loss of function
Rheumatoid arthritis • chronic, systemic inflammatory disease; autoimmune disorderjoints, myocardium, vessels, muscles are involved, esp. joints - proliferative synovitis, articular cartilage destruction, progressive articular immobilization • 1% in population, frequention of disorder during aging is greateronset in all age groups, in all races and social groups • charakteristics: rheumatoid nodules (central zone of fibrinoid necrosis surrounded by a prominent rim of fibroblasts, epitheloid histiocytes, lymphocytes, plasma cells)localization: skin; lungs, spleen, pericardium, myocardium, heart valves, aorta, etc. • hallmark of diagnosis: estimation of rheumatoid factor (RF) in bloodautoantibody against Fc fragment of IgG (it is also IgA or IgM in character)
Rheumatoid arthritis - pathogenesis • RA is triggered by exposure of an immunogenetically susceptible host to an arthritogenic microbial antigensinitiation of acute arthritis by continuing autoimmune reaction activation of CD4+ helper T-cells; local release of inflammatory mediators and cytokines destruction of the joints • the first step requires • susceptible host – most patients are HLA-DR4 and/or HLA-DR1 positive • microbial/viral antigen – EBV, retroviruses, parvoviruses; Borrelia, Mycoplasma • normal lymphocyte function: antigen present cells stimulation CD4+(the amount of CD8+ decreases) B-lymfo stimulationRF release • neoangiogenesis – consequence of cytokine release from macrophages – a/b FGFinduction of endothelial cells to invasion into articular cavity and to creation of capillaries – joint destruction • RF (character IgM) bounds complement release of mediators from mast cellsmicrothrombi creation
Rheumatoid arthritis • proliferative, destructive synovitis; great amount of PMNC in synovia (release of adhesive molecules from endothelial cells + C5a, leucotrien B4, PAF migration of PMNC into articular cavity • PMNC (after phagocytosis of IC) – release of proteinases, collagenases, elastases collagene destruction • IL-1, TNFα acute phase protein synthesis • immunocomplexes start of coagulative cascade fibrinjoint destruction bradykinin (involved tissue), histamin (mast cells), serotonin (thrombocytes) increase of vessel permeability • diagnosis: morning stifting, arthritis in three or more joint areas, symmetric arthritis, rheumatoid nodules, serum rheumatoid factor, radiographic changes (joint effusion, juxtaarticular osteopenia, narrowing of the joint space, loss of articular cartilage)
Bone • inorganic component (60%) – prevalently calcium hydroxyapatitestore of 99% of all calcium, 85% of phosphorus, 65% of Na and Mg • organic component proteins in matrix proteins produced by osteoblasts progenitor cells osteoblasts osteroclasts osteocytes • cell restoration and activation is controlled by a/b FGF, PDGF, IGF-1, TGFβ
progenitor cells (osteoprogenitor cells) pluripotent mesenchymal stem cells osteoblastsosteoblasts- bone surface function: creation of new bone (synthesis and release of proteins necessary to formation of bone matrix an bone mineralization)receptors for PTH, PTHrP, vitamin D3, estrogenes, cytokinesosteoblasts osteocytesosteocytes – reciprocal communication by net of canalliculi transfer of membrane potentials, substrates control local Ca and P concentrationosteoclasts – derived from CFU-GM (tissue macrophages) differentiation of osteoclasts is realized by influenced of IL-1, IL-3, IL-11, TNF, GM-CSF, M-CSFduring growth bone modeling (prevalently due to action of osteoblastsafter cartilage closure remodeling (synchronous action of osteoblasts and osteoclasts)primary bone resorption stimulators effect on osteoblast receptors; osteoblasts release proteins activating osteoclasts
Control of bone metabolism • PTH, vitamin D3, calcitonin • PTH – if decline of blood Ca level increasing of synthesis and release evokes mobilization of Ca from bone, increases osteoclasts activity; in the kidney – greater resorption of Ca creation of 1,25 (OH)2 vitamin D3 • vitamin D3 – food intake, synthesis in the skin after UV irradiation 25-OH vit. D3 osteoid mineralization 24,25 (OH)2 vit. D3 osteoblast stimulation 1,25 (OH)2 vit. D3 intestinal Ca resorption, osteoblast stimulation • calcitonin, PTHrP (source: thyroid parafollicular cells) lowering of Ca level in hypercalcemia; osteoblast inhibition
Disturbances of bone tissue • inherited malformations non-development of some of fingers, ribs etc. creation of superabundant fingers, ribs; syndactilia, arachnodactylia • majority of inherited malformations gene mutation in homeobox HOX D disturbance of transcriptional factors • achondroplasia(disease of growth cartilage) base: mutation of gene encoding FGFR3 clinical: normal lenght of torso, head enlargement, shortening of limbs intelligence, reproductive efficiency are normal
Osteoporosis • atrophy of the bone – equal decrease both inorganic and organic part of bone – normal decrease of bone tissue after puberty = 0,5% / year • etiologic factors • age– progenitor cells reduction of the proliferative ability, decreaseof osteoblasts -- senile osteoporosis • reduced physical activitymechanical forces are important stimuli for normal bone remodeling importance in long term laying patients • calcium nutritional state– a) decreased intake, b) low resorbtion, c) increased loss (kidney) • hormonal influences – low production of estrogenes, higher production of glucocorticoids (decreased production of estrogenes release of IL-1, IL-6, TNFα indirect stimulation of osteoclasts (posmenopausal osteoporosis) • clinical: isolated or multiple fractures, deformity (spine)
Rickets and osteomalacia • characterization: defect in matrix mineralization due to lack of vitamin D3 or some disturbance in its metabolism • in children – rachitisin adults – osteomalaciadefect in mineralization of osteoid • lack of vitamine hypocalcemia release of PTH mobiliza-tion of Ca from bone • in rachitis – deformities, in osteomalacia – fractures • considerably high production of PTHmicrofractures, bone cysts, hemorhage in bones (brown colour of bones and surrounding connective tissue – deposition of hemosiderin) osteitis fibrosa cystica (Recklinghausen´s disease
Osteogenesis imperfecta • disturbance of α1 or α2 chain of collagene (type I) • bones, joints, eyes, ears, skin, teeth are affected (structures rich in type I collagen) • shortening ofα1 chain – blue sclerae, hearing loss, outstanding bone fragility death in utero or within days of birth α2 chain – outstanding bone fragility, blue sclerae, dental imperfectionin all forms of osteogenesis imperfecta too little bone
Osteopetrosis • disease caused by osteoclasts dysfunction disturbance of bone remodeling, difuse bone sclerotization • thickenig of bone, narrowed of BM cavity • pathogenesis 1) carbonic anhydrase deficiency (lack of H+ needed for solubilization of bone matrix) 2) osteoclast cannot generate superoxid • cause: mutation of gene encoding M-CSF • clinical signs:malignant autosomal recessive form: fractures, anemia, hydrocephalypospartum mortality – in surviving: cranial nerve problems, extramedullar hemopoiesisbenign autosomal dominant form: repeated (micro)fractures, mild anemia,mild cranial nerve problems)
Paget disease (osteitis deformans) • “collage of matrix madness“ • repetitive and overlapping sequence of1) initial osteolytic state (outstanding activity of osteoclast)2) mixed osteoclastic-osteoblastic stage – at the end is predominance of osteoblastic activity3) burn-out quiescent osteosclerosis • these stages are evident in the bone • cause: slow virus infection (paramyxovirus) osteoclast, CFU-GM, MNC infection synthesis and release of IL-6 (it is produced by osteoblasts powerful stimulation of osteoclasts) • clinical signs: one or more bones may be involved. Thickening of bone esp. of cortex, decrease of bone marrow cavity.painbone overgrowth in the cranofacial skeleton leontiasis ossea
Renal osteodystrophy • term renal osteodystrophy describes all of skeletal changes in chronic renal disease:increased osteoclastic bone resorptiondelayed matrix mineralizationosteosclerosisgrowth retardationosteoporosis • pathogenesis hyperphosphatemia secondary hyperparathyroidism inductionof osteoclastic activityhypocalcemia due to low production of 1,25(OH)2 vit. D3 PTHinduction of osteoclastic activitymetabolic acidosisrelease of calcium from the matrix • clinical signs: osteomalacia (mimicking osteitis fibrosa cystica)osteoporosis; deposition of masses of amyloid in bone (amyloid is formed from β2-microglobulin – e.g. it is increased after long-term hemodialysis)
Urémie Renální osteodystrofie Zvýšená aktivita příšt. tělísek způsobující charakteristickou subperiostální resorpci Lebka „sůl a pepř“