Download
1 / 39
390 likes | 495 Views
Childhood Thyroid Cancer in Belarus Following the Chernobyl Accident. Yu. Demidchik , M. Fridman. Part 1. THYROID CANCER STATISTICS Two etiological forms (radiogenic and sporadic) High incidence in children within the first decade after Chernobyl

E N D
Childhood Thyroid Cancer in Belarus Following the Chernobyl Accident Yu. Demidchik, M. Fridman
Part 1 THYROID CANCER STATISTICS • Two etiological forms (radiogenic and sporadic) • High incidence in children within the first decade after Chernobyl • Since 2001, only sporadic cases were diagnosed • Prevalence of PTC • Follicular, medullary or anaplastic carcinomas are extremely rare • Recently, about 50% of patients present micro carcinomas at diagnosis
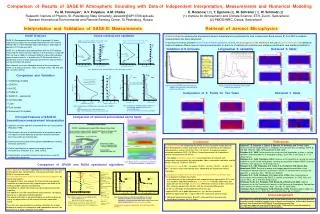
Crude incidence and mortality for thyroid cancer(:100 000) (1965–2013) In total, 23795 patients were diagnosed from 1970 Mortality rates are available only since 1990 (1747 patients died within 1990-2013)
Crude incidence and mortality for thyroid cancerin males (:100 000) (1970–2013)
Crude incidence and mortality for thyroid cancerin females (:100 000) (1970–2013) Incidence increased by 8 times as compared with 1986
Crude incidence (: 100 000) for thyroid cancer in different regions (1970–2013)
Crude incidence(: 100 000) for thyroid cancer depending on age group (1970–2013)
Part 2 THYROID CANCER IN CHILDREN • 1418 cases of thyroid carcinomas (under 19 y.o.) were diagnosed in the period from 1986 and 2010 (all histological forms). • Of them, 1169 are available for assessment. • The individuals born after April, 1987 were considered as non-radiogenic.
The beginning of significant increase of incidence in exposed to 131I • Aged over 19 • Aged under 18
Childhood crude incidence (: 100 000) for thyroid cancer in different regions (1970-2013)
Adolescent crude incidence (: 100 000) for thyroid cancer in different regions (1970-2013)
Post Chernobyl thyroid cancer cases in children depending on place of residence at the time of Chernobyl accident (1986-2005)
POST CHERNOBYL (RADIOGENIC) PATIENTS-1 Total number of cases: 936 (non-PTC cases and irradiated previously for other malignancies excluding) • Females: 600 (64.1%) • Males: 336 (35.9%) • Ratio: 1.8:1 Age: 4.2 – 18.99 (13.6) • Under 10 y.o.: 157 (16.8%) • 11-14 y.o.: 364 (38.9%) • 15-18 y.o.: 415 (44.3%)
POST CHERNOBYL (RADIOGENIC) PATIENTS-2 • Tumor size • Average: 14.4 mm (range 1-124 mm) • From 1 to 5 mm: 84 cases • From 6 to 10 mm: 302 • Above 11 mm: 550 (58.8%) • Involved lymph nodes • N0 :246 (26.3%) • N1a:309 (33.0%) • N1b:381 (40.7%) (41.2%) (73.7%)
POST CHERNOBYL (RADIOGENIC) PATIENTS-3 • Distant metastases at primary diagnostics — 104 (11.1%). • Extrathyroidalextent – 387 (41.3%). !Note! In 262 (28.0%), the capsular involvement is not assessed. • Multifocality – 60 (6.4%)
POST CHERNOBYL (RADIOGENIC) PATIENTS-4 • Pathological features • Classical PTC – 360 (38.5%) • Follicular variant – 292 (31.2%) • Diffuse sclerosing variant – 73 (7.8%) • Tall cell – 65 (6.9%) • Clear cell – 10 (1.1%) • Solid – 136 (14.5%) • Involved blood vessels – 176 (18.8%) • Involved lymphatic vessels – 790 (84.4%)
POST CHERNOBYL (RADIOGENIC) PATIENTS-5 • Thyroid background – 148 (15.8%), including • Autoimmune thyroiditis – 72 • Follicular adenoma – 20 • Nodular goiter – 56 • Dominant architectonics • Papillary – 300 (32.1%) • Follicular – 453 (48.4%) • Solid – 183 (19.6%)
CONCLUSION#1 Post Chernobyl (radiogenic) PTC is frequently extrathyroidal. The tumor size in largest measurement is usually small but associated with high frequency of neck lymph nodes involvement (73.7%) and distant metastases (11.1%)
CONCLUSION#2 • Local or regional recurrence after thyroidectomy is likely for 5 years and distant metastases can spread for 6 years. • In cases of surgery other than thyroidectomy, the probability of local or regional recurrence is high in any terms of follow-up. • Distant metastases can be detected within 10 years after partial thyroid resections.
CONCLUSION#3 • To avoid local or regional recurrence in children and adolescents with PTC, primary surgery has to be based on total thyroidectomy followed by radioiodine therapy depending on indications • Despite this strategy, distant metastases can appear 5-6 years after surgery being associated with tumor peculiarities: involved blood vessels, patients’ age and refusal from radioiodine
Part 3 SPORADIC THYROID CANCER IN CHILDREN
No clear evidence of geographical factor in sporadic cases (n=210; 1986–2010)
Differences between sporadic and radiogenic cancer Sporadic carcinomas were significantly more common on abnormal thyroid background. In sporadic cases, lung metastases are significantly less common as compared with radiogenic carcinomas (2 cases; 1.4%).
Causes of death in 26 pts • Cause specific death: 2 • Acute leukemia: 2 • Gastric cancer: 1 (totally 10 pts have second cancer) • Accidents and traumatic lesions: 6 • Suicide: 7 • Surgical complications: 1 • Lung fibrosis: 1 • Liver cirrhosis: 1 • Cardiac failure: 1 +2 sporadic • Mixedema: 1 • Brain infarction: 1
CONCLUSION#4 The prognosis in childhood and adolescent thyroid cancer is favorable.
Acknowledgment • Dr. Yu. Averkin • Prof. D. Williams • Prof. K. W. Schmid • Prof. C. Reiners • Dr. M. Fridman • O. Krasko