Download

1 / 23
260 likes | 419 Views
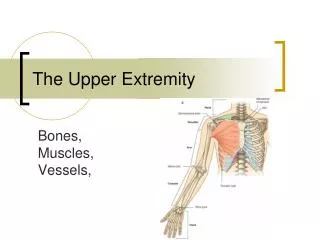
Upper Extremity. Types of fractures. Incomplete-torus and greenstick Complete Closed fracture Open fracture-ortho emergency-IV antibiotics-tetanus-irrigate and debride Pathologic fracture Stress fracture. Salter-Harris Classification Type I-fracture through epiphyseal plate

E N D
Types of fractures • Incomplete-torus and greenstick • Complete • Closed fracture • Open fracture-ortho emergency-IV antibiotics-tetanus-irrigate and debride • Pathologic fracture • Stress fracture
Salter-Harris Classification • Type I-fracture through epiphyseal plate • Type II-fracture of metaphysis with extension through the epiphyseal plate • Type III-fracture of epephysis with extension into the epiphyseal plate • Type IV-fracture through the metaphysis, epiphysis and epiphyseaal plate • Type V-crush fracture of the epiphyseal plate
Elbow • Post. Fat pad-never normal on x-ray. Represents swelling of the joint capsule and probably fx. • Ant. Fat pad-a small one may be present on normal x ray. If superior and anteriorly displaced, could represent a fracture. • Anterior humeral line-line down the ant. surface of the humerus normally transects ther middle of the capitellum. With a supracondylar extension fracture the line may transect the ant. 1/3 or completely ant. to the capitellum
Supracondylar extension fracture-most common-FOOSH-potential injury of the brachial artery and median nerve-may result in compartment syndrome • Treatment-ortho consult-post. splint with the arm at 90 degrees if non displaced. Displaced require surgical reduction. If vascular compromise, try to reduce once in the ED
Supracondylar Flexion fractures-direct blow posterior flexed elbow-distal humerus is displaced anteriorly-ulnar nerve injury is the most common complication • Treatment-nondisplaced-immobilization with early ortho follow up—Displaced-emergent ortho consult for reduction and pinning
Olecranon fractures-MOI direct blow to point of elbow or FOOSH with elbow flexion • Nondisplaced—elbow immobilized in 30 degree flexion-fractures with 2mm displacement ORIF • Condylar fractures • Articular surface-trochlea and capitellum • Nonarticular surface-medial and lateral epicondyle
Condylar fractures usually involve the articular and nonarticular surfaces • Treatment-nondisplaced or minimally displaced, immobilize in 90 degrees of elbow flexion with forearm suppination
Elbow dislocations Posterior-most common-fall on extended and abducted arm-arm held in 45 degree flexion and posterior olecranon Injuries of the ulnar and median nerve are common Suspect brachial artery injury Reduce under conscious sedation. Distal traction at wrist with humerus immobilization. Flex the elbow with posterior pressure to the distal humerus. Post reduction films.
Anterior dislocations-MOI-elbow flexed with a blow to the olecranon. • Forearm is elongated and supinated • Higher incidence of vascular damage • Treatment- immobilize the humerus with in-line traction to the wrist and downward/backward pressure on the proximal forearm
Radial head subluxation-occurs in children generally <5y.o. • MOI-longitudinal traction on the hand or forearm with arm in pronation • Presents with arm hanging and unwilling to move it; elbow flexed and arm in passive pronation • Xrays are usually normal • Reduce by placing the thumb on the radial head and supinating the forearm and flexing the elbow
Radial head fractures-FOOSH-look for bulging ant. fat pad or a post. fat pad sign. • Nondisplaced fractures treated with sling immobilization • Displaced fractures immobilized in long arm post splint with ortho consult
Galeazzi fracture-fracture of the distal radial shaft with a distal radioulnar dislocation • Monteggia’s fracture-fracture of the proximal third of the ulna with dislocation fo the radial head • With fractures of both radius and ulna, they are usually displaced and a high suspicion of compartment syndrome is warrented.
Shoulder • Sternoclavicular joint injuries • 1st degree-partial tear of the sternoclavicular and costoclavicular ligaments; without clavicular subluxation-Treatment-sling • 2nd degree-complete tear of the SC ligament plus partial tear of the costoclavicular ligament with subluxation of the clavicle from the manubrium-Treatment-clavicular strap or sling with ortho F/U • 3rd degree-Post. Dislocations require OR. For others, put a roll between the shoulders while supine. Extend, abduct, and apply traction to the ipsilateral arm while pushing or pulling with a towel clip on the clavicle. Place in clavicle strap or sling and refer to ortho
Acromioclavicular separation • 1st degree (type I)-partial tear of the AC ligament without subluxation of the clavicle • 2nd degree (type II)-complete tear of the AC ligament with subluxation of the clavicle: the coracoclavicular ligament is stretched or incompletely torn • 3rd degree (type III)-complete tears of both AC and coracoclavicular ligaments with dislocation of the clavicle • 4th degree (type IV, V, VI)-significant displacement of the distal clavicle posteriorly (type IV), superiorly (Type V), and inferiorly (type VI) as well as injury to the deltoid or trapezius muscle.
Radiographic findings • Type 1—AC joint is normal-Treatment sling for 1-2 weeks • Type 2-distance b/t the acromion and the inferior/distal clavicle is increased by one half or less the width of the clavicle-treatment sling and ortho referral • Type 3-distance between the acromion and the distal aspect of the clavicle is increased by at least one half the width of the clavicle. Also increased distance b/t the distal clavicle and the coracoid process is increased. Treatment-immobilize v. surgery • Type 4-6-surgical fixation is definitive
Shoulder dislocations-should get AP and Y view x-rays • Axillary lateral view helps differentiate anterior from posterior dislocations. • Anterior-most common • MOI-abduction, extension and external rotation • Arm is held in abduction and external rotation
Hill-Sachs deformity-compression fracture as the humeral head impacts the glenoid rim • Bankart lesion-fracture of the anterior glenoid lip • Axillary nerve injury can occur and will present with sensory loss over the lateral deltoid • Must check radial pulse and examine for expanding hematoma as this can represent an axillary artery injury.
Posterior dislocations usually occur due to seizure or electrocution. • MOI-fall forward on a flexed, adducted and internally rotated arm • Presents with internal rotation and adducted • Most can be reduced in the ED
Reduction techniques for anterior dislocation • Stimson or hanging-weight • Scapular manipulation • Traction-countertraction • External rotation • Milch forward elevation
Posterior dislocations-axial traction and then the humeral head is pushed forward-consult ortho first • Always recheck neurovascular exam and post reduction x-rays
Tintinalli • Rosens • WWW