Download
1 / 54
550 likes | 733 Views
Sam Tsemberis, PhD CEO Pathways to Housing, National Juliana Walker, LCSW Housing First Coordinator Amarillo VA. Housing First: Ending Homelessness and Systems Change. Special Thanks. Thank you to Vince Kane, the former Director of the National Center on Homelessness Among Veterans

E N D
Sam Tsemberis, PhDCEO Pathways to Housing, National Juliana Walker, LCSWHousing First CoordinatorAmarillo VA Housing First: Ending Homelessness and Systems Change
Special Thanks Thank you to Vince Kane, the former Director of the National Center on Homelessness Among Veterans Thank you to Susan Langer for coordinating this presentation.
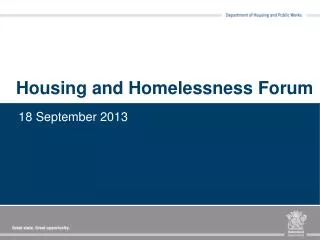
Housing First HUD-VASH Demographics of Veterans Served in 14-Site Demonstration Project
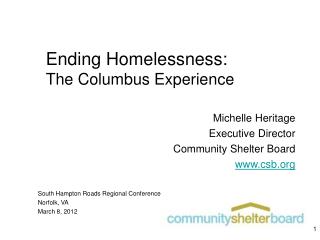
Housing: Stability – by Program Percentage of time housed
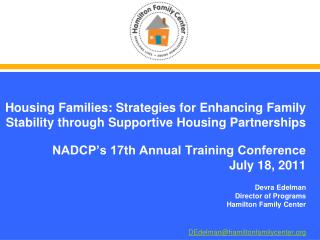
Housing First HUD-VASH Average VHA Healthcare Cost Pre- and Post-Housing Placement (N=402) $36,407 ~36% reduction in VHA costs
Where We Began The Traditional System of Care The Continuum of Care or the Linear Residential Treatment Model
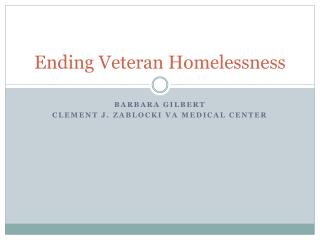
Traditional Treatment then Housing System Permanent housing Transitional housing Level of independence Shelter placement Homeless Treatment compliance + psychiatric stability + abstinence
Where do people end up?TAU about 40% success Institutional Circuit 60% ill-served
What Most Veterans WantHousing First Direct Access to apartment of your own Permanent housing Transitional housing Shelter placement Ongoing, flexible support Harm Reduction Homeless
Pathways’Housing First! Housing is a right not a reward for ‘good’ behavior
HF at the VA Has 2 Components 1. Housing / Rental Subsidy – for HUD-VASH this is most often a tenant based Section 8 Voucher ₊ 2. Services – Provided by the HUD-VASH team and the larger VAMC
Housing First: Clearly Defined Complex Clinical Intervention • Pathways Housing First Program Fidelity • 1. Consumer Choice in Housing & Services • 2. Separation of Housing & Services • 3. Service Array (matches client needs) • 4. Service Philosophy (Recovery Focus) • 5. Program Structure
Personal Paradigm Shift • Change in philosophy (client directed) • Change in view of people served (capabilities, strengths based) • Change in service location (veteran’s home/community) • Change in power relationships (client determines the sequence, type and intensity of service) • Change in professional practice (team practice vs individual practitioner; collaboration, transparency) • ** Change based on clinical and research evidence – HF is an evidence based practice, high program fidelity- better results
PRICIPLE I: Consumer Choice “Real choice is not only having the ability to pick from a number of predetermined options; it is also about having the power to add that which you as a consumer want, to those options.” -Ron Coleman, author of Working Toward Recovery “The freedom, they have given me…They’re not controlling my life; they’re helping me to better my life” -PtH client
Separation of Housing and Services • Different standards for success in housing and treatment • Relapse is followed with support and return to a home • Loss of housing ≠ loss of clinical team • Program commitment is to the personnot the housing • Graduation – services walk away; person stays home
Who is involved in Finding Housing? • Participant • Support and treatment services team • Housing staff • External housing agency • Community landlords • Building superintendents • Housing Authority
The 3rd partner in HF programs - Community Landlords • Without a wide network of landlords the program is not possible • A reliable income stream • Access to support services to address problems • Can reduce vacancy rates • Evokes altruistic feelings and a sense of giving back to the community
Tenancy Related Services • Team provides services and support in all aspects of choosing, getting and keeping housing • Supports participants to maintain independent, permanent, housing (their own apartment) • Housing stability seen as crucial to the recovery process
Key to Successful Tenancy: Responsiveness • Quick and effective communication • Include all parties: • Participants • Team members • Landlords and community • Team has a two part role: • 1st Advocate for consumer • 2nd Maintain relationship with Landlord and community
Working As A Team Services Provided in Housing First How the Services Are Provided
Working As A Team • Why Use A Team Approach? • Shared Caseloads • Working on Blended Teams
SERVICES ARRAY 3: MATCH CLIENT NEEDS “NO WRONG DOOR” Friends & Family ACT Team Direct services; trans-disciplinary practice ICM Teams Some direct services; brokerage model Blended Teams- Incorporates Elements of ACT and ICM Participants Immediate access; client-directed Employment/ education Spiritual Income Entitlements/ Legal Wellness/ Nutrition CLIENT PEER SUPPORT RN/MD Arts / Creativity HOUSING Addiction Mental Health
SERVICE modalities ACT or ICM: Matching the level of services to the person’s needs Assertive Community Treatment • High Need: ACTis a multidisciplinary team and provides support and services directly Intensive Case-management • Moderate Need: ICMcase management team provides support and brokers services • Services provided in the participant’s home or community • Group meetings offered at offices or other community settings • Off site and on-call services 7-24 • All teams use a recovery orientation
Staff Positions • Interdisciplinary team members work on all aspects of participant’s needs but are also trained in a specialty • Specialists roles and functions • Peer specialists • Housing Specialist • Nurse • Social Workers • Addiction Specialists • Psychiatrist /Nurse Practitioner • All services can be provided in the Veterans home
Why teams are a good fit for housing first • Community-based model • Provide services in the community • Follow the consumer • Can provide services directly to individuals who are either unwilling or unable to seek clinic-based services
Benefits of A Team Based Approach USE A TEAM BASED INTERVENTION FOR ICM TEAMS: • Improves staff coverage • Geographic coverage, Crisis management • Relationship management (rotating workers or roles) • Multiple inputs on all consumers (complex cases) • Shared responsibility, and ‘got your back” • Team meetings, peer supervision and support • Reinforce core practice values Strengths-Based Case Management:Values, Knowledge and Skills
Team Communication Daily Schedule- Lists activities that need to be carried out for each participant and assigns team members to each. Finalized by Team Leader and Shift Manager. Monthly Home Visit Schedule: Home visits should be scheduled between case manager and client and noted on client and consumers calendars. Boards/Logs – Have 3 boards/Logs; One tracks this week’s activities, second tracks the next week’s, and third will track the month’s. Can be tracked on shared web calendars but should also display in prominent place in the office. Census report- List of all participants, telephone number and address- especially as people start to move in.
Team Communication: The Huddle • Morning meetings to review status and goals of the client • Every team member attends or leaves detailed notes to be read • Team’s daily activities are organized and coordinated • Tabling of participants who need longer discussion • Have clear structure and stay focused on the client’s goals How are you participating and creating the vision?
After Hours • Veterans must know who to call after hours • The team must have close communication with after-hours services to ensure strong continuity of care
Team Leader: Leader/Team member: Directs, supervises, leads and supports staff in a manner that is consistent with the recovery mission. Attends to the health of the team as a whole. Leads morning and service planning meetings. Teacher/Supporter: Helps team members learn how to prioritize Provides information about basic counseling techniques to team members that need it Provides individual, group and team supervision Clinician: Dedicates a percentage of time to direct consumer services Shares Clinical Responsibility with the MD or NP
Housing Specialists • Housing specialist and clinical staff and consumer meet together during initial engagement phase • Housing specialist works with community landlords/real estate listings, networks to identify suitable apartment and hopefully neighborhood of choice • Housing Specialist can act as a liaison between Landlords and Clinical staff
Peer Specialists • Individuals with lived experience representing their recovery and experience as expertise like other team experts • Peer specialist is not a ‘junior case manager’ • Can provides a qualitatively different conversation and support to clients (e.g., going together to AA or NA) • Inspirational role model for clients and staff • Strong representative of clients point of view and life style • Peer specialists have often been identified as key people in other’s journey of recovery
Common Challenges of Service Providers in HF Programs • How do you maintain choice driven approach? • With a team approach who is ultimately responsible for the plan? • How do you balance the work that involves both specialist and generalist functions? • How do you manage re-housing and evictions? • How do you manage time? • How do you prevent becoming crisis driven? • How do you maintain team cohesion and “esprit de corps”?
Recovery and Harm Reduction What Are Recovery Focused Service? What is Harm Reduction? How Does Harm Reduction Work In Housing First?
4. Recovery Orientation Person Centered Capability focus Inter-personal (you are an active agent in the treatment and outcome)
Harm Reduction and Housing First Harm Reduction (HR)is an integral part of program philosophy in HF Since housing individuals without requiring treatment or sobriety we are immediately involved in the practice of Harm Reduction HR is using practical and creative strategies to reduce the negative consequences associated with any behaviors that can be problematic
Harm Reduction and Housing First HR is not limited to working with addiction It seeks to reduce the risks of any harmful behaviors (psychiatric symptoms, self destructive high risk behaviors) HR is what you do until the client is ready to engage in treatment HR is compatible with client directed services HR is compatible with trauma informed care
Harm Reduction Core Principle: Accept People as They Are • Trauma filled history • Current or continued trauma • Constantly judged by others • Constantly judging themselves • Undiagnosed Mental Illness • Low Self Worth • Feeling of Hopelessness • Feelings of Powerlessness • Poverty • Many want to rid themselves of their addiction
Housing First and Harm Reduction Recovery-Focused: • Emphasizes and supports the potential for recovery • Understands recovery is a moving journey, not a set outcome • Involves: hope, stability (housing, financial, health, safety), self worth, support, healthy relationships, empowerment, coping skills, social inclusion, meaning • Success is consumer’s Strengths-Based: • Focus is on strengths not psychopathology or previous failures • Empowering consumers
Harm Reduction in Housing First • Meeting a person where they are at • Consumer chooses goal; Team supports • Relapse is followed with support (not housing loss or discharge) • Harm Reduction is defined by Consumer • Their goals; Not ours • Their view of success; Not ours • Does not have to be steps toward sobriety* *Must be able to support consumer directed sobriety
Working with the Sufferer, not the Disease This work is not undertaken or presented as an expert’s knowledge of the life a person should lead. At the core, this work is not to heal the drug addict or mentally ill. A conviction that all people must be treated with dignity and worth and all people have the ability to achieve the life they desire given the supportand encouragement in achieving their chosen goals. Do not regard addiction as a sign of weakness, but a sign of suffering. Recovery is defined by the sufferer. Recovery is within the reach of all.
Lessons Learned Three Take Away’s