Download
1 / 49
490 likes | 649 Views
Plant and brain cannabinoids: major players in physiology. Raphael Mechoulam. Beit Dagan, January 2007. LOH 2003.

E N D
Plant and brain cannabinoids:major players in physiology. Raphael Mechoulam Beit Dagan, January 2007 LOH 2003
Gan-zi-gun-nu – the drug that takes away the mindAzallu – hand of ghost, poison of all limbs (neurological diseases?)Qunnabu – used in religious rites
Pliny, the Elder (79 AD): The roots boiled in water ease cramped joints, gout too and similar violent pain.Dioscorides (90 AD): The sodden root when placed on inflammations sooths them, eliminates edema and disperses obdurate matter above inflammed joints. LOH 2003
For the relief of certain kinds of pain, I believe, there is no more useful medicine than Cannabis within our reach. J. Russell Reynolds, Archives of Medicine, Vol 2, 154, 1859
CH CH 3 3 CH O H 3 O H OH HO C H 5 11 O C H 5 11 HO C H 5 11 9 9 cannabidiol (CBD) D D cannabigerol (CBG) -tetrahydrocannabinol ( -THC) (Mechoulam and Shvo, 1963) (Gaoni and Mechoulam, 1964) (Gaoni and Mechoulam, 1964) CH 3 O C H O 5 11 C H 5 11 O H O H O H O C H 5 11 cannabichromene (CBC) cannabicyclol (CBL) (Claussen et al., 1966; (Crombie et al., 1968) cannabinol (CBN) Mechoulam and Gaoni, 1966) (Adams et al., 1940) Representative natural cannabinoids LOH 2003
CH 3 O H O D9-tetrahydrocannabinol (D9-THC) Gaoni and Mechoulam: J.Amer.Chem.Soc. 86, 1646 (1964) Mechoulam and Shvo: Tetrahedron 19,2073 (1963)
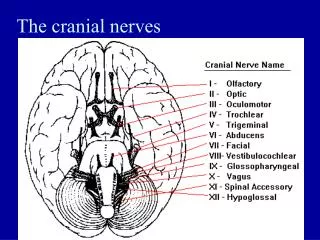
Brain regions in which cannabinoid receptors are abundant Basal ganglia Movement control Substantia nigra pars reticulata Enteropeduncular nucleus Globus pallidus Putamen Cerebellum Body-movement coordination Hippocampus Learning and memory, stress Cerebral cortex, especially cingulate, frontal, and parietal regions Higher cognitive function Intrabulbar anterior commissure Link between cerebral hemispheres Nucleus accumbens Reward pathway
Agonists (e.g. THC, anandamide) Cannabinoid receptor G G (-) (-) AC AC K+ Potassium channels open K+ (-) Calcium entry blocked [cAMP] Ca2+ [Ca2+] Decreased release of neurotransmitters
What do endocannabinoids do? “Relax, eat, sleep, forget and protect” Di Marzo, 1998
Physiological systems and conditions affected by endocannabinds (a partial list) Anxiety Inflammation Appetite/feeding Memory Blood pressure Mood Bone formation Movement Cerebral blood flow Neuroprotection Digestive system Pain Emesis and nausea Reproduction Immune system Stress LOH 2004
Levels of 2-AG in mouse brain after CHI ««« 120 110 100 90 80 «« «« « 70 60 concentration of 2-AG(nM/gr) 50 40 30 20 10 0 control 15 min 1 h 4 h 8 h 24 h Time after CHI Anova with Tukey post-test:P<0.0001, F=36.01 ««« -P<0.001 vs. control Nature 413, 527 (2001) «« -P<0.01 vs. control « -P<0.05 vs. control
Effect of exogenous 2-AG on edema after CHI 81.5 « -P<0.05 vs.CHI 80.5 « « « 79.5 % water 78.5 77.5 76.5 sham CHI 0.1 5 10 (mg/kg) Effect of exogenous 2-AG on recovery after CHI * 3.0 2.5 2.0 DNSS (improvement) 1.5 1.0 0.5 0.0 CHI 0.1 5 10 (mg/kg)
2-AG Reduces Infarct Volume 24 h After CHI 15.0 2-AG control 12.5 2-AG 5 mg/kg 10.0 * 7.5 infarct volume(%) 5.0 control 2.5 0.0 2-AG (5 mg/kg) control n=7 n=9 unpaired t-test, P=0.0 3
Brain injury 2-AG glutamate cytokines, ROS Vasoconstrictors (e.g. ET-1, Thromboxane) neuronal & glial cell death cerebral ischemia cerebroprotection
Aldosterone Progesteron Costicosteroids Digitalis Corticosteroids Androgens Estrogens
O H O C N H C O O H arachidonoyl serine
Inhibition of TNFa production by 2-AG In vitro 200 150 production (S50 units) 100 50 a TNF 0 0 0.05 0.1 1 5 10 50 2-AG (mg/ml) LOH 2004 Eur.J.Pharmacol. 406, R5-R7 (2000)
Inhibition of TNFa production by 2-AG in mice In vivo 2000 1500 LPS LPS + 2-AG in serum (S50 units) LPS + 2-AG + +2-LG + 2-PG 1000 a 500 TNF 0 LOH 2004
Synovium is the most critical site of cytokine production in arthritis. Synovial cells from arthritic mice spontaneously produce large amounts of TNF when cultured in vitro.Cells from arthritic mice which had been treated with CBD produced significantly less (50%) TNF. LOH 2003
Cannabidiol (i.p.), acute control 2.5 mg/kg 5 mg/kg 5 10 mg/kg 20 mg/kg 4 Clinical score 3 2 1 0 0 1 3 5 7 9 11 Days after onset of arthritis LOH 2003
Mean change in weight from baseline in patients with AIDS treated with dronabinol (THC) and placebo (Beal et al., 1995) Dronabinol Placebo
Effect of anandamide on food intake (16 mouse in each group).
50 ** *** *** 40 30 Per cent freezing (60 s tone) 20 …… 10 ……… 0 Co d1 d3 d6 d2 CS CS CS CS Experimental day LOH 2004
The endogenous cannabinoid system could represent a therapeutic target for the treatment of diseases associated with inappropriate retention of aversive memories or inadequate responses to aversive situations, such as post-traumatic stress disorders, phobias, and certain forms of chronic pain. LOH 2004
Cannabinoids and anxiety. 1. In animal models as well as in limited clinical trials cannabidiol has been shown to lower anxiety. Mechanism unknown. 2. Blocking of anandamide hydrolysis in vivo (rats) enhances anandamide levels in brain and lowers anxiety. This effect is blocked by endocannabinoid antagonists.
Cannabinoids and schizophrenia. 1. Large doses of cannabis (particularly if they lack cannabidiol) may cause a psychotic state resembling psychosis. 2. In schizophrenic patients cannabis use may worsen positive symptoms. 3. Heavy use of cannabis may precipitate schizophrenia in susceptible individuals. Frequent cannabis use was associated with 6 fold increase of in high risk individuals (family history). 4. Increase in density of CB1 receptors in several brain areas in postmortem schizophrenic brains. Two fold increase of anandamide levels in CSF of patients.
Cannabidiol treatment of positive schizophrenia. High doses of the non psychoactive Cannabis constituent cannabidiol have shown effectiveness in the treatment of schizophrenics (lowering of positive effects). Mechanism – unknown.
Endocannabinoids and depression. Although at low doses cannabis may enhance mood it is not antidepressive. A selective inhibitor of the enzyme which causes endocannabinoid hydrolysis (in vivo) exerts potent anti-depressant effects in the rat forced swim test.
Hepatic encephalopathy. Hepatic encephalopathy (HE) is a neuropsychiatric syndrome due to liver disease. It is the feature that defines prognosis in acute liver injury. 1. In a mouse model of HE (produced by the toxin thioacetamide) 2-AG levels are enhanced in the brain. 2. Administration of either 2-AG or the specific CB2 agonist HU-308 improves a neurological score, activity, cognitive function. 3. A specific CB2 receptor antagonist blocks these effects.
Alzheimer’s disease Compared to currently approved drugs prescribed for the treatment of Alzheimer’s disease, THC is considerably superior inhibitor of Ab aggregation and thus cannabinoid molecules may directly impact the progression of this debilitating disease. (Eubanks et al., Mol. Pharmac. 2006)
Collaboration in Israel Jerusalem Prof. L. Hanuš Prof. E. Fride Dr. W. A. Devane Dr. A. Breuer Dr. S. Ben-Shabat D. Panikashvili G. Milman N. Kogan Y. Maor Jerusalem Prof. E. Shohami Prof. R. Gallily Prof. E. Berry Prof. M. Schlesinger Dr. Y. Avraham Haifa Prof. A. Mandelbaum Rehovot Prof. Z. Vogel Tel Hashomer Dr. S. Almog Dr. A. Gopher LOH 2003
Collaboration abroad • Aberdeen • R. Pertwee • Bonn • M. Karsak • Zimmer • Brno • Šulcová • Greece • C. Simeonidou • Richmond • B. Martin • H. Lichtman • Canada • L. A. Parker • Bethesda • G. Kunos • M. Spatz • Napoli • V. Di Marzo • Rome • M. Maccarrone • Siberia • L. Maslov • London • M. Feldmann • M. Malfait • P. F. Sumariwalla LOH 2003