Download
1 / 39
400 likes | 629 Views
Men ought to know that from the brain, and from the brain only, arise our pleasures, joy, laughter and jests, as well as our sorrows, pains, griefs, and tears. Hippocrates (c 400 B.C.) . Epilepsy, brain and mind Dr Niall Pender Clinical Neuropsychologist

E N D
Men ought to know that from the brain, and from the brain only, arise our pleasures, joy, laughter and jests, as well as our sorrows, pains, griefs, and tears.Hippocrates (c 400 B.C.)
Epilepsy, brain and mind Dr Niall Pender Clinical Neuropsychologist Beaumont Hospital & National Neuroscience Centre Dublin, Ireland
Important facts about brains and epilepsy • Brains are complex organs that work mainly on electricity; • Different parts of the brain manage and control different activities…but they are all inter-connected; • Brain and mind are indistinguishable! • There is a relationship between epilepsy, brain function, psychological state (mind) and the world around us. • “The brain is a little saline pool that acts as a conductor, and it runs on electricity.” • Judith Hooper and Dick Teresi (from The Three-Pound Universe, 1986)
Vicious Cycle in Epilepsy Adapted from: Lorig et al, 2006
How are epilepsy, brain and mind related? • There is a relationship between brain (damage) and behaviour (thought and emotion); • AND • These difficulties can affect individuals (and their families); AND • We can identify and manage these difficulties.
Introduction • Epilepsy is defined by a group of conditions characterised by recurrent provoked seizures: • A seizure occurs when the brain's nerve cells misfire and generate a sudden, uncontrolled surge of electrical activity in the brain. • The epilepsies are common • 1-2% prevalence • 50 million worldwide • Cause is often unknown • ~ 60 % seizure free without side effects • Often only treating symptoms with medication • Associated cognitive and emotional side effects
Classification • Generalised • Primary (genetic) • Absence • JME • GMUA • Symptomatic • West syndrome • LGS • PME • Partial • Genetic • Benign rolandic • Benign occipital • Acquired (Lesional/ Non-lesional) • Temporal • Frontal • Occipital • Parietal
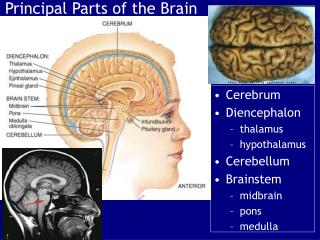
Epilepsy, brain and mind • Location of functions in the brain; • Lateralisation of functions to sides of brain; • Damage to brain structures can alter brain function; • Behavioural state; • Cognitive functioning; • Emotional state; • Specific Tests can identify these skills and abilities.
FACTS • The adult human brain weighs ~3lbs; • It represents ~2% of total body weight; • But uses 20% of total energy; • There are ~100billion neurons; • Neuron, dendrites and an axon. • There are three layers of covering called..meninges • Dura mater, arachnoid mater and pia mater • LOC occurs 8-10 seconds after loss of blood to the brain; brain damage after 4 minutes
The frontal lobe is defined as the area rostral (in front) of the central sulcus and above the lateral fissure. The parietal lobe lies between the central sulcus rostrally and an imaginary line extending from the parieto-occipital sulcus caudally. The occipital lobe is situated caudal to the same imaginary line of the parieto-occipital sulcus. The temporal lobe is located under the lateral fissure and rostral to the imaginary line extending from the parieto-occipital sulcus. Lobes of the brain • The frontal lobes make up 41% of total cerebral cortex volume;
Psychological Consequences of Epilepsy: Epilepsy and the mind!
Different forms of epilepsy have different symptoms • Temporal lobe epilepsy is most often associated with cognitive and behavioural changes due to the importance of these structures…genetic factors; • However, other forms of epilepsy such as primary generalised epilepsy have been shown to have more subtle but equally disabling difficulties…attention
Cognitive • These skills can be affected in epilepsy and can have a significant impact on education, occupation and day to day life. • The most commonly reported changes are in attention and concentration as well as memory. • Others can report word finding difficulties and especially fatigue. • Poor thinking speed can also reported
Why? • Our brains have a number of systems that enable us to take in and use information which can easily be disrupted but…….“forgetting things is normal”; • Sometimes in epilepsy these skills can be disrupted making it harder for people to learn and use information. • Seizures often arise in the memory centres and these can disrupt learning and remembering. • Some anti-convulsants can also cause poor memory
Neuropsychological examination • General abilities: • IQ measures and verbal .v. non-verbal differences help us examine the consequences of brain changes • Memory: • Verbal v non-verbal recall and recognition memory; Learning • Executive processing: • Behavioural control, problem solving, reasoning • Language functioning: • Perceptual ability: • Thinking speed
Attention and memory • Memory lapses are common; • Attention a key gateway to memory but is easily impaired; • It is a system to allow us to prioritise activity and monitor performance. • Poor attention leads to poor memory; • Seizures, medication, alcohol, reduced sleep, stress/anxiety all affect attention; • Day to day difficulties experienced but on testing no deficits apparent….attentional loss
Epilepsy and intellectual function • Epilepsy is common in individuals with an Intellectual Disability • The frequency of epilepsy in people with a learning disability is higher than in the general population. About 30% of people with a learning disability also have epilepsy. In people with a severe learning disability at least 50% also have epilepsy. • The more severe someone's learning disability is, the more likely it is that they will also have epilepsy.
Epilepsy and psychological functions Can anti-epileptic medication cause side effects or changes in behaviour? • Some people may react badly to their anti-epileptic medication. A brain that has been damaged is more prone to possible side effects. Sometimes side effects include poor attention, restlessness and slowed or unsteady movement. These may be difficult to tell apart from the signs of the underlying damage to the brain. If someone is not able to communicate what they are feeling, this may result in withdrawn or challenging behaviour. Can epilepsy impair cognitive functioning? • Cognitive difficulties in people with learning disabilities are usually due to the underlying brain damage that caused the epilepsy rather than the epilepsy itself. If the seizures are well controlled and the drug regime is kept simple, further cognitive difficulties are less likely. If seizures are poorly controlled or very frequent they may affect the person's overall quality of life. If seizure control increases these difficulties may also improve.
Epilepsy and depression • Major depressive disorder in 8-48% with an average of ~29%(Herman et al, 2000); • Weigartz et al. (1999) 30% major depressive disorder, 25% dysthymic disorder;
Epilepsy and depression (2) • Reaction to epilepsy label; • Reaction to social/family/lifestyle difficulties; • Seizure related phenomena; • Some depression unrelated directly to seizures, but possibly to increased frequency; • Depressive symptoms related to other mental illnesses.
Epilepsy and anxiety • 25-33% of people with drug resistant epilepsy suffer anxiety • Higher incidence of social phobia in epilepsy sufferers
Non-Epileptic Seizures or Non-Epileptic Attack Disorder (NEAD) • Betts (1991): “a sudden disruptive change in a person’s behaviour which is usually time-limited, and which resembles, or is mistaken for, epilepsy, but which does not have the characteristic electrophysiological changes in the brain detectable by EEG, which accompanies a true epileptic seizure”. • Imparting the diagnosis of NEAD is the first step to successful treatment • New diagnosis must lead into psychological treatment ideally within the same service • Flexible approach to treatment as responses to diagnosis will vary Thanks to: Dr Gillian Fortune
NEAD: Categories & Co-morbidity • ORGANIC NEAD: Cardiovascular; Cerebrovascular; Migraine (espec. Basilar); Alcohol-related; Post-anaesthetic; Pre-eclampsia • PSYCHOGENIC NEAD: Conversion Disorder • Psychological/Emotional/Personality causes • Psychological Conditions Associated with NEAs • Depression 25-60% • Anxiety disorders 12-50% • Personality disorder 30-60% • Other Conversion disorder 30-80% • e.g. numbness, weakness, blindness, fainting, paralysis • Alper et al (95) • 25% of NEAs accounted for by Panic disorder, psychosis, ADHD, depersonalisation disorder
Vicious Cycle in Epilepsy Adapted from: Lorig et al, 2006
Obstacles to self-management Knowledge Family support Seizures types & Medications Attitudes Care & Lifestyle Skills & behaviours
What can we do? • Awareness and identification of problems are first; • Considering epilepsy as a serious health problem that must be addressed; • Improving self-management of epilepsy • Medication; • Seizure factors; • Lifestyle; • Improved coping
Better self management comes from: • Freedom in decision making; • Authority; • Support; • Responsibility; • Education is vital to this process • Need more educational programmes for people at different stages in the illness of epilepsy Living Well With Epilepsy II (2003)
Fatigue • Fatigue is one of the most commonly reported symptoms in neurological conditions; • It is also the most concerning aspect to patients; • Patients describe: • Tiredness • Weakness; • Inability to generate muscle force; • Inability to sustain mental or physical performance. • Related to CNS dysfunction, poor immune regulation, chronic illness effects
Important factors to consider when working cognitive difficulties • Do not overload person with lots of demands • Little and often is important • Information processing can be slow….don’t rush • Reduce distraction where possible • Patients fatigue very easily….give rests • Use diaries, memory aids, calendars and others such as phone to support your memory
Other changes: The old favourites-lifestyle! • Nutrition • Exercise for fitness & general well-being • Medication, discuss worries with team • Relaxation to manage anxiety • Education on the illness and skills • Memory, emotion etc • Communicating fears and worries
Overall • Learning to self-manage is not about isolation and going it alone! • It is about taking over the management of your illness and learning to break the vicious cycle to give you more control over an often unpredictable illness: • This method has been effective in other chronic illness and is part of a general focus on many lifestyle factors in health