Download
1 / 37
430 likes | 796 Views
Rhabdoviruses HUMAN RABIES. Professor Sudheer Kher. DEFINITION. Rabies is an acute, progressive encephalomyelitis The case to fatality rate is the highest of any infectious disease One of the oldest described diseases The leading viral zoonosis as regards global public health significance.

E N D
RhabdovirusesHUMAN RABIES Professor Sudheer Kher
DEFINITION • Rabies is an acute, progressive encephalomyelitis • The case to fatality rate is the highest of any infectious disease • One of the oldest described diseases • The leading viral zoonosis as regards global public health significance
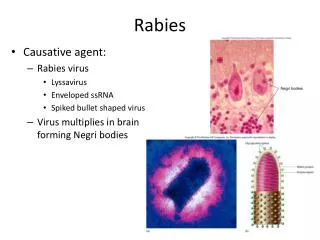
Etiology - RABIES VIRUS • Rhabdoviridae family • Lyssavirus genus • helical, enveloped • ss RNA, -VE sense • Bullet shaped
BURDEN • More than ~55,000 human rabies deaths per year • Most occur in developing countries • Millions of human exposures per year • The domestic dog is the single most important animal reservoir • Wildlife important, especially in developed countries
RABIES HOSTS • All warm-blooded vertebrates are susceptible to experimental infection • Mammals are the natural hosts of rabies • Reservoirs consist of the Carnivora (canids, skunks, raccoons, mongoose, etc.) and Chiroptera (bats)
ANIMAL RESERVOIRs • DOGS • MONGOOSE (main reservoir in RSA in the wild) • SURICATE • JACKAL • BAT (some evidence to suggest carrier status and droplet infection) • FOX (in Europe) • SKUNKS, RACCOONS (in USA) • SEMI-WILD DOGS (in Natal)
TRANSMISSION • BITE - USUAL ROUTE • CORNEAL AND OTHER TRANSPLANTS • MUCOSAL MEMBRANES, WOUND • AEROSOL (RARE)
HUMAN RABIES • HUMAN-TO-HUMAN • surgically - via transplants • no direct human-to-human ever documented
RABIES PATHOGENESIS • Virus is transmitted via bite • Agents are highly neurotropic • Enter peripheral nerves • Centripetal travel by retrograde flow in axoplasm of nerves to CNS • Replicate in brain • Centrifugal flow to innervated organs, including the portal of exit, the salivary glands • Viral excretion in saliva
Note: No viremia Murray et al., Medical Microbiology
CLINICAL STAGES • Incubation Period (range = ~<7 days to >6 years; average is ~4-6 weeks) • Prodromal Phase (Non-specific signs) • Acute Neurological Phase • Coma • Death (recovery from rabies?)
SYMPTOMS • Variable, often misdiagnosed • Tingling, paresthesia at bite site • Fever, headache, malaise, anorexia • Nausea, vomiting, myalgia, hydrophobia • Confusion, hallucinations, seizures, paralysis • Coma, respiratory failure, death
Clinical Presentation • Furious Rabies • Headache, fever, irritability, restlessness and anxiety. muscle pains, salivation and vomiting. • After a few days to a week the patient may experience a stage of excitement and be wracked with painful muscle spasms, triggered sometimes by swallowing of saliva or water. Hence they drool and learn to fear water (* Hydrophobia). • The patients are also excessively sensitive to air blown on the face. The stage of excitement lasts only a few days before the patient lapses into coma and death. • Once clinical disease manifests, there is a rapid, relentless progression to invariable death, despite all treatment.
Clinical Presentation • Dumb Rabies Starts in the same way, but instead of progressing into excitement, the subject retreats steadily and quietly downhill, with someparalysis, to death. Rabies diagnosis may easily be missed.
Dumb rabies • Seen in occasionally in animals like dogs. The animal is paralysed, not aggressive. Saliva is infective. • Carrier state in animals – Not common but has been reported. • Implication – Vaccination essential even after exposure to non-rabid dogs/animals.
RABIES RECOVERY? • Five historical human case recoveries, after vaccination, but before illness onset • Only one documented unvaccinated human survivor after clinical presentation
Fixed Vs Street Virus • Freshly isolated virus from human/animals is called Street virus. Highly virulent. • Virus after serial passages in rabbit brain / tissue cultures is called as Fixed virus. Less virulence and hence used for vaccine production.
RABIES DIAGNOSIS • Based upon history of animal exposure and typical neurological clinical signs • Postmortem demonstration of viral antigen in CNS is gold standard • In humans, antemortem detection of virus or viral amplicons, antibodies, or antigens (sera, csf, saliva, nuchal biopsy)
By assessment of: 1.Bite - Geographical area, type of animal, severity and site of bite. 2.Animal Live - observe in cage: If survives > 8 days, then NOT rabies. Dead - brain sent to Ref Virology Lab - Negri bodies - IFA virus isolation Man Live - difficult diagnosis - clinical picture, skin biopsy, corneal impression (antibodies only appear very late) Dead - brain sent to Virology Lab "Negri bodies" in cytoplasm of brain cells; immunofluorescence virus isolation DIAGNOSIS
DIAGNOSIS • neutralizing antibodies in serum or CSF • direct fluorescence antibody • nuchal biopsy (nape of neck), brain biopsy • RT-PCR saliva • post-mortem staining of brain slice • Negri bodies (not always seen)
The Negri body • Inclusion body • Stain used Seller’s stain – Basic fuchsin + Methylene blue in methanol. • 3-27 µ, intracytoplasmic, round or oval, purplish pink structures with inner basophilic granules.
FLUORESCENT ANTI-RABIES NUCLEOPROTEIN ANTIBODY Rabies virus infected Uninfected CDC
Rabies virus infected Uninfected CDC
Rabies virus infected - Negri body - note dark blue basophilic granules (Seller’s stain) CDC
RABIES EXPOSURE • Bite (common cause) • Non-bite (rarely causes rabies) • Contacts with blood, urine, feces, etc. are not considered exposure • Many scenarios, such as merely seeing a rabid animal, being in the same room, petting, etc., are not considered grounds for prophylaxis A small bat bite on a finger
PROPHYLAXIS • Pre-exposure Vaccination • Postexposure Prophylaxis (PEP)
RABIES BIOLOGICALS • Rabies Vaccines (for pre- and PEP) • Rabies immune globulin (only in PEP)
Available vaccines • Neural Vaccines – 5% Sheep brain suspension • Semple – Inactivated by phenol • BPL – Inactivated β propiolactone • Mouse Infant brain • Non-neural – • Egg vaccine Duck / Chick Embryo • Cell culture • Human diploid cell vaccine (HDCV) _ Commonly used. • Purified Vero cell culture vaccine (PVCV) • Purified chick embryo cell vaccine (PCECV)
PRE-EXPOSURE VACCINATION • Provided to subjects at risk before occupational or vocational exposure to rabies • VETERINARIANS AND STAFF • WILDLIFE OFFICERS ETC LIKELY TO CONTACT RABID ANIMALS • TRAVELERS LIKELY TO BE AT RISK • RABIES RESEARCH WORKERS • Simplifies postexposure management
PRE-EXPOSURE VACCINATION • Vaccine given on days 0, 7, and 21 or 28 • Serology occurs every 6 months to 2 years (if remaining at risk) • If antibody titer not adequate, administer a single booster dose • If ever exposed, give a vaccine dose on days 0 and 3, regardless of titer
POSTEXPOSURE PROPHYLAXIS • Provided to subjects after rabies exposure • Consists of wound care, rabies immune globulin, and vaccine • If prompt and proper, survival virtually assured
POSTEXPOSURE PROPHYLAXIS • Wash lesions well with soap and water (tetanus booster ad hoc) • Infiltrate rabies immune globulin (20 IU/kg) into and around the margin of the bites • Administer vaccine on days 0,3,7,14, and 28
POSTEXPOSURE PROPHYLAXIS • Urgency rather than emergency, per se • Depends in part upon the animal species, exposure details, rapidity of diagnostic testing, and epidemiology of rabies in the local area • Consultation with knowledgeable public health officials should be routine
POST-EXPOSURE PROPHYLAXIS • CLEAN WOUND • Include soap and water, alcohol or benzyl- alkonium chloride etc. No suturing. • STATE HEALTH DEPARTMENT • determine risk, examine animal (if available) • VACCINATION • Human Diploid Cell Vaccine • fetal rhesus lung cell vaccine • Purified Chicken Embryo Cell vaccine • HUMAN RABIES IMMUNE GLOBULIN • HRIG • infiltrate up to half around wound, rest IM
RABIES IMMUNE GLOBULIN • Two Human Rabies Immune Globulins in the USA: HyperRabTM S/D Imogam® Rabies-HT • Both supplied in vials at ~ 150 IU/ml
ADVERSE REACTIONS • PEP should not be interrupted because of local or mild systemic adverse reactions • Use of anti-inflammatory, antihistaminic, and antipyretic agents suggested • Serious systemic, anaphylactic, or neuroparalytic reactions are rare