Download
1 / 50
510 likes | 675 Views
Managing ISOLATED SYSTOLIC HYPERTENION in the Elderly. Ass. Prof. Roland KASSAB Head of Division of Cardiology Hotel-Dieu de France, Beirut 12 April 2003. ISH. Definition Prevalence Pathophysiology Risk Statification Outcomes Studies Therapy. DEFINITION.

E N D
Managing ISOLATED SYSTOLIC HYPERTENION in the Elderly Ass. Prof. Roland KASSAB Head of Division of CardiologyHotel-Dieu de France, Beirut 12 April 2003
ISH • Definition • Prevalence • Pathophysiology • Risk Statification • Outcomes Studies • Therapy
DEFINITION According to JNC-VI and WHO/ISH: SBP ≥ 140 mmHg, DBP < 90 mmHg Grade 1: SBP < 160 mmHg Subgr. borderline SBP < 150 mmHg Grade 2: SBP < 180 mmHg Grade 3: SBP ≥ 180 mmHg
JNC VI Guidelines for Definition and Dg of HTA • Defined as SBP ≥ 140, DBP ≥ 90mmHg, or taking any antihypertensive medication. ■ When SBP and DBP fall into different categories, the Higher one is used to classify the BP. ■ Measurements are based on the average of 2 ormore BP readings at each of 2 or more visits after the initial screening. ■ Measurements must be taken with equipment that meets certification criteria, and in a standardized fashion.
Definition of HTA (JNC VI) • Hypertension is defined as consistent readings 140/90mm Hg in young and older adults • Classification of BP for adults age 18 and older The Sixth Report of the Joint National Committee on Prevention, Detection, Evaluation and Treatment of High Blood Pressure. November 1997. NIH publication 98-4080
PREVALENCE Old Definition: ≥ 160 / < 90 • Latest Definition: ≥140/<90 : little data • Prevalence of ISH with age • Most common type of HTA in the elderly • Most preval. type of untreated HTA ≥ 60 y.
Hypertension in the Elderly(>60 Years) in Spain • Prevalence of arterial hypertension: 68.3% • Prevalence of ISH in untreated hypertensives: 71.6% Banegas J et al. J Hypertens (submitted)
NHANES III 4% 10% 18% 28% 27% 13% 100% 80% 60% 40% 20% 0% Frequency of treatment Failures by HTN subtype (%) <40 40-49 50-59 60-69 70-79 80+ Age (y) ISHS/DH IDH Franklin et al, Hypertension 2001
Framingham: Prevalence of Isolated Systolic Hypertension in the Elderly* Women Men Isolated Diastolic Hypertension Isolated Systolic Hypertension Combined Hypertension *Age range: 65-89 years Wilking SV et al. JAMA.1988;260:3451-3455.
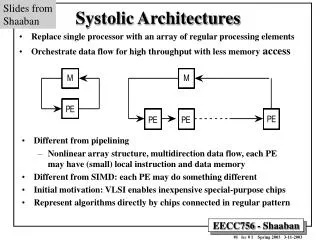
PATHOPHYSIOLOGY B.P. = Cardiac Output X Periph. Resistance ( Qc ) ( R ) ↑ B.P. ↔ ↑ Qc or ↑ R
Characteristics of Hypertension in the Elderly • Increased arterial stiffness • Altered renal function • Frequent diabetes and hyperlipidemia • Frequent association with CV disease and heart failure • Frequent occurrence with other complications and disease states (polypharmacy, noncompliance are common issues)
The Effects of Age on Blood Pressure • Systolic BP rises continuously with age • Diastolic BP rises continuously until age 60-70 years • It falls thereafter as a consequence of increased arterial stiffness • Pulse pressure increases continuously with age
PATHOPHYSIOLOGY Stiffened aorta Increased pulse-wave velocity More stroke volume returned to aorta in systole rather than diastole SBP augmented further, DBP reduced Potential harm of reducing DBP (J curve) Smulyan H, Safar ME. Ann Intern Med. 2000;132:233-237.
RISK STRATIFICATION Components of Risk Stratification: JNC VI: MAJOR RISK FACTORS ♥ Smoking ♥ Dyslipidemia ♥ Diabetes Mellitus ♥ Age ≥ 60 y. ♥ Sex ( ♂, post-menopausal ♀ ) ♥ Family history or Co-vx disease:♀< 65y, ♂< 55y
RISK STRATIFICATION TARGET ORGAN DAMAGE ( TOD ) ♥ Heart Disease: LVH, Angina or previous MI, prior CABG, HF ♥ Stroke or TIA ♥ Nephropathy ♥ PAD ♥ Retinopathy.
Systolic vs Diastolic Blood Pressure as Predictors of Cardiovascular Outcomes • Systolic blood pressure (SBP) is a stronger predictor of future cardiovascular events than diastolic blood pressure (DBP)1 • Patients with a combination of hypertension and diabetes and/or older patients benefit most from well-controlled systolic blood pressure2 • In addition, pulse pressure (PP = SBP minus DBP) is increasingly seen as an independent predictor of risk for coronary artery disease3 1. Neaton JD, Wentworth D. Arch Intern Med. 1992;152:56-64. 2. Lee ML et al. Ann Epidemiol. 1999;9:101-107. 3. Franklin SS et al. Circulation.1999;100:354-360.
48.3 CAD Death Rate per 10,000 Person-Years 37.4 80.6 31.0 34.7 43.8 25.5 23.8 38.1 24.6 20.6 16.9 25.3 100+ 13.9 25.2 10.3 24.9 12.8 11.8 90-99 12.6 80-89 8.8 11.8 160+ 75-79 8.5 70-74 140-159 9.2 <70 Diastolic BP(mm Hg) 120-139 <120 Systolic BP(mm Hg) Effect of Systolic Blood Pressure and Diastolic Blood Pressure on Coronary Heart Disease Mortality: MRFIT Adapted from Neaton JD, Wentworth D. Arch Intern Med. 1992;152:56-64.
Framingham Study: At Any Level of Systolic BP, Pulse Pressure* is a Strong Predictor of Cardiovascular Events 3.0 2.5 SBP 170 mm Hg(P = 0.0487) N = 1,924 2.0 Coronary Artery Disease Hazard Ratio SBP 150 mm Hg(P = 0.0194) 1.5 SBP 130 mm Hg(P = 0.0086) 1.0 SBP 110 mm Hg(P = 0.2076) 0.5 30 40 50 60 70 80 90 100 110 Pulse Pressure (mm Hg) *Pulse pressure = systolic blood pressure (SBP) minus diastolic blood pressure (DBP). Franklin SS et al. Circulation. 1999;100:354-360.
Major Studies of Pharmacologic Tt in ISH ►► SHEP ►► Syst-EUR ►► Syst-China ►► ARBs studies: LIFE sub-study OUTCOMES STUDIES
_ _ _ _ _ _ _ + + + + + + + Indicates those with BP not reduced to or below goal Indicates those with BP reduced to or below goal The Systolic Hypertension in the Elderly Program (SHEP) Trial Design Atenolol 50 mg C 25 mg Atenolol 25 mg C 25 mg Chlorthalidone 25 mg (C2) Atenolol 25 mg C 25 mg C25 mg Chlorthalidone 12.5 mg (C1) Placebo A2 Placebo C2 Placebo A1 Placebo C2 IC BV1 Placebo C2 Placebo A1 Placebo C2 Placebo Placebo C2 Placebo C1 Randomization Week 16 24 - 4 - 2 0 8 IC = initial contact; BV1 = baseline visit 1. SHEP Cooperative Research Group. J Clin Epidemiol. 1988;41:1197-1208. SHEP Cooperative Research Group. JAMA. 1991;265:3255-3264.
The Systolic Hypertension in Europe (Syst-Eur) Trial Design N = 4,695 Placebo • Outcome Events • Death • Stroke • Retinal changes • Myocardial infarction • Heart failure • Dissecting aneurysm • Serum creatinine 4mg % • Entry criteria • Age: >60 years • Sitting SBP 160 mm Hg Sitting DBP <95 mm Hg • Standing SBP: 140 mm Hg • Informed consent Placebo Active Treatment Nitrendipine 10-40 mg Enalapril 5-20 mg Hydrochlorothiazide 12.5-25 mg • Double Blind • Visit every 3 months • Duration: 5 years • Single blind • Visit monthly • Duration: 3-4 months Amery A et al. Aging. 1991;3:287-302.Staessen JA et al. Lancet. 1997;350:757-764.
Relative Risk Reduction (%) EntryBP AllCVD Agent N Age Stroke CAD CHF Diuretic ±beta-blocker 4,736 60 SHEP 171/77 -36 -27 -55 -32 60 Long-actingDHP CCB(nitrendipine) Syst-Eur 4,695 174/86 -42 -26 -29 -31 Landmark Trials in Isolated Systolic Hypertension CAD = coronary artery disease; CHF = congestive heart failure; CVD = cardiovascular disease. SHEP Cooperative Research Group. JAMA. 1991;265:3255-3264. Staessen JA et al. Lancet. 1997;350:757-764.
6 5 4 3 2 1 0 0 12 24 36 48 Isolated Systolic Hypertension and Stroke Risk Reduction Cumulative Rate of Fatal and Nonfatal Stroke SHEP Syst-Eur 10 Placebo Placebo Diuretic beta-blocker 8 Nitrendipine Cumulative Stroke Rate per 100 Participants 42% Reduction in Events (P = 0.003) 36% Reduction at 5 Years (P <0.0003) 6 4 2 0 0 12 24 36 48 60 Follow-up (months) Follow-up (months) SHEP Cooperative Research Group. JAMA. 1991;265:3255-3264. Staessen JA et al. Lancet. 1997;350:757-764.
T T T R LIFE: ISH Study Design and Dosing Titration to target blood pressure: <140/<90 mm Hg Other Antihyper-tensive Medications* N = 1326 Hydrochlorothiazide 12.5 mg HCTZ 12.5 to 25 mg Losartan 50 mgorAtenolol 50 mg Losartan 100 mgorAtenolol 100 mg Placebo Day 14 Day 1 Month 2 Month 4 Month 6 *Other antihypertensives excluding ACE-Is, ARBs, beta-blockers; T = titration; R = randomization. Kjeldsen SE et al. JAMA. 2002;288:1491-1498.
58.8% 60 55.1% 45 32.3% 30 25.5% 12.1% 15 10.1% 3.6% 2.6% 0 50 or 100 mg + HCTZ add-on D/C therapy 100 mg+ add-on 50 or 100 mgmonotherapy Losartan (n = 660) Atenolol (n = 666) LIFE Isolated Systolic Hypertension Substudy: Combination or Monotherapy at End of Titration Percent HCTZ = hydrochlorothiazide; D/C = discontinued. Adapted from Kjeldsen SE et al. JAMA. 2002;288:1491-1498.
LIFE: Primary Composite End Point in Patients With Isolated Systolic Hypertension Primary Composite End Point Total Mortality 18 18 16 16 Relative Risk = 0.72 (95% Cl, 0.53-1.00) P = 0.046 14 14 12 12 Patients WithFirst Event (%) 10 10 8 8 6 6 4 4 Relative Risk = 0.75 (95% Cl, 0.56-1.01 P = 0.06 2 2 0 0 0 6 12 18 24 30 36 42 48 54 60 66 0 6 12 18 24 30 36 42 48 54 60 66 Study Month Study Month Atenolol Losartan Blood pressure reduction was virtually identical in losartan (28/9 mm Hg) and atenolol (28/9 mm Hg) arms. Kjeldsen SE et al. JAMA. 2002;288:1491-1498.
LIFE: Components of the Composite Primary End Point in Patients With Isolated Systolic Hypertension Stroke 10 8 6 4 2 Relative Risk = 0.60 (95% Cl, 0.38-0.92) P = 0.02 0 0 12 24 36 48 60 Study Month Cardiovascular Mortality 10 10 Study Month 8 8 6 6 Patients (%) 4 4 2 2 Relative Risk = 0.54 (95% Cl, 0.34-0.87) P = 0.01 0 0 0 12 24 36 48 60 Study Month Myocardial Infarction Patients (%) Patients (%) Relative Risk = 0.89 (95% Cl, 0.55-1.44) P = 0.64 0 12 24 36 48 60 Study Month Atenolol Losartan Kjeldsen SE et al. JAMA. 2002;288:1491-1498.
LIFE Isolated Systolic Hypertension Substudy: Conclusions • Most patients with ISH received combination treatment withhydrochlorothiazide (58.8% in the losartan group and 55.1% in the atenolol group) • >70% of patients that finished the trial received combination therapy • Reductions of 28 mm Hg in systolic blood pressure and 9 mm Hg in diastolic blood pressure were achieved in the losartan and the atenolol groups • At the same levels of blood pressure control, losartan significantly reduced stroke risk and overall cardiovascular mortality but not the risk of suffering a myocardial infarction • The impact of ARB + HCTZ treatment on cardiac morbidity and mortality alone needs to be further evaluated in future trials Kjeldsen SE et al. JAMA. 2002;288:1491-1498.
Reduction of BP in Patients65 Years With Valsartan Change from Baseline (mm Hg) *P <0.001, valsartan vs placebo. Neutel JM et al. Clin Ther. 2000;22:961-969.
THERAPY As with any therapy, the pragmatic 4 W questions must be answered: WHY ? WHEN ? WHO ? WHAT ?
WHY ? • According to the previous trials, in ISH: ►Treatment >> Placebo ► Significant ↓ Cardio-vx Morbidity and Mortality ■ Benefits of ↓ Systolic B.P. and PulsePressure
835 N = 15,693 734 Nonfatal Events Deaths 656 647 Individuals Affected (N) 392 387 373 342 327 329 293 279 244 193 136 100 Tx Tx C Tx C Tx C Tx C C Stroke CAD All CVEvents TotalMortality Non-CV Mortality Reduction in Odds (%) 23% P <0.001 30% P <0.0001 26% P <0.0001 13% P <0.02 Meta-Analysis: Reduction of CV Events in Treated vs Untreated Patients With Isolated Systolic Hypertension Tx = treatment; C = control (untreated); CAD = coronary artery disease; CV = cardiovascular. Staessen JA et al. Lancet. 2000;355:865-872.
WHEN ? • Appropriate Diagnosis of ISH • Institute Lifestyle Modifications: ♥ Weight loss ♥ Salt restriction ♥ Exercise program ♥ Reduction of alcohol intake ■ If HT persists, institute Drug Treatment.
WHO ? • All patients with ISH • Risks higher in smokers and diabetic pts • Tight control of diabetes, cessation of smoking +++ • In the previous trials, ↓ in absolute risk from all major Co-vx events almost twice in diabetic sub-group.
WHAT ? Start with a Single Agent: ► Dose should be ↓ in elderly: ≈ ½ dose ► Long-acting formulations preferred for better compliance ► Low-dose combinations helpful: ↓ S.E. ► Titrate ↑ and/or add 2nd agent if goal not reached after 1 to 2 months.
PHARMACOTHERAPY • Avoid agents ↔ profound ↓ in Diastolic BP ( Pulse Pressure ++) • Avoid agents causing serious Side Effects • Theoretic advantage of vaso-dilators improving arterial compliance • Recommendations of JNC VI :
DIURETICS • First-line Tt of ISH in elderly ( SHEP ) • Good control often seen at low doses • Thiazides: Diuretics of choice • Thiazide diuretics seem to be > to Beta- blockers in pts with ISH.
CA CHANNEL BLOCKERS • Improve arterial compliance • Well tolerated in comorbid conditions • Low-dose, slow-release agents • First-line Tt in Syst-EUR and Syst-China • Significant ↓ in key end points • Benefit over Diuretics: ↓ rate of dementia (by 50%) in treated pts.
BETA BLOCKERS • First-line Tt in combination with Thiazides • Starting agents alone in some conditions: ♥ Tachycardia ♥ CAD ♥ Prior MI N.B. BB with intrinsec Σ activity or combined α blocker activity may be more effective
ACEI and ARBs ► Numerous advantages: ♥ ↓ Proteinuria ♥ Slow renal disease ♥ Improve systolic dysfunction ♥ ↓ SBP in pts with ISH ► Indicated in ISH + HF, Proteinuria, Diabetic Nephropathy.. → Before the LIFE ISH sub-study
ARBs • After the LIFE: ISH sub-study: ♥ First trial demonstrating superiority of one anti-HT agent vs another ♥ Losartan > Atenolol in ↓ Stroke and Cardio-vx Mortality ■New Recommendations of JNC including ARBs (Losartan) as First-line Tt??
NITRATES • Vaso-dilatory action on conduit vx • May alter timing of reflected pr. waves • P.O.: ↓ SBP without sign. changes in DBP • Well tolerated in elderly • Advantageous in pts with angina • No large and randomised trials.
α ADRENERGIC BLOCKERS NOT recommended as first-line agents by JNC VI: ↑ Co-vx events ↑ Congestive HF Compared with other agents.
RECOMMENDATION In all cases, decisions and regimens must be institued and tailored in accord with a patient’s other comorbid conditions and responses to medication. THANK YOU FOR YOUR ATTENTION