Download
1 / 61
610 likes | 615 Views
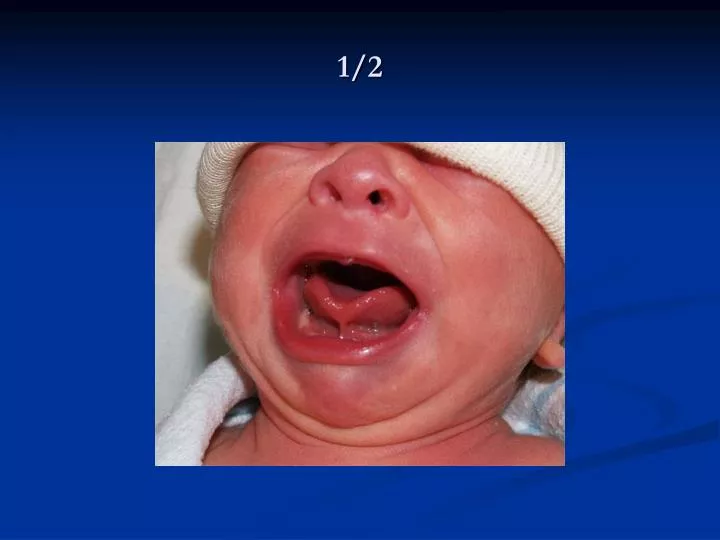
1/2. 2/2. Ankyloglossia. 4% of newborns. Many babies with this condition can breastfeed without difficulty. In more severe cases, can prevent tongue protrusion and/or cause a V-shaped fissure in the tip of the tongue, especially with crying.

E N D
Ankyloglossia 4% of newborns. Many babies with this condition can breastfeed without difficulty. In more severe cases, can prevent tongue protrusion and/or cause a V-shaped fissure in the tip of the tongue, especially with crying. A frenotomy may be indicated when a tight frenulum makes latching on difficult. Outcome of speech in infants identified at birth is controversial.
Supernumerary Nipple (Polythelia) Found along the mammary line. They may be single or multiple, unilateral or bilateral. It is an insignificant finding.
Due to effects of maternal estrogen. Lasts < 1 week. No clinical concern. White discharge referred to as “witch’s milk” may be present. Breast Hypertrophy
Skin Tag The nipple area is a common location for small skin tags. They are typically very small. Do not need to be removed.
Case 6 • You are seeing a patient for the first time at his 2 week well child visit. The mother asks you if the bulge coming from his chest is normal…
Prominent Xiphoid Does not represent an abnormality. Frequently observed finding in newborns. With time, this becomes less noticeable.
Wharton’s Jelly Cyst • Also known as a “false cyst” of the cord. • It is a fluid-filled sac that can be related to a swelling of the Wharton's jelly. • Up to 20% of infants with this condition have associated anomalies.
Case 6 • The mother of a newborn is concerned about a bulge in the baby’s abdomen every time he cries or has a bowel movement. What should you tell her?
Diastasis Recti Vertical bulge down the midline of the abdomen. Seen in many newborns when intra-abdominal pressure increases. Caused by a relative weakness of the fascia between the two rectus abdominus muscles. Disappears with time.
Umbilical Hernia • Due to incomplete closure of the fascia of the umbilical ring. • More common in African Americans and LBW infants. • Usually close spontaneously by age 3 (most common by age 1). • Surgical correction needed if incarceration occurs or if hernia very large and persists past age 3.
Case 7 • As you are examining a newborn at his 2 week well child check, you notice drainage coming from the umbilicus. The umbilical stump fell off several minutes prior to your exam. What do you tell the mother?
A spot of blood or a slight amount of moist, yellow material is normal after cord separation. Any bleeding or discharge that persists should be evaluated.
Penile Pearl • “Pearls” may be found in different locations in the newborn. • Also known as Epstein pearls in the mouth. • The tip of the foreskin is common location. • Small, firm, white nodule that contains keratin. • Spontaneous exfoliation and resolution. • Not a contraindication for circumcision.
Hydrocele • Fluid filled sac in the tunica vaginalis of the testis or along the spermatic cord. • Resolve spontaneously.
Normal Female Genitalia • White vaginal discharge as well as bloody discharge is normal in the newborn period. • Due to maternal androgens. • Also seen is vermix along the interior surface of the labia majora. • No special cleaning is needed.
Sucking Blister Blister created by the infant sucking on his extremity while in utero. Solitary lesion that occur only in areas accessible to the infant’s mouth. Resolve spontaneously.
Postaxial Polydactyly Next to 5th digit of hand or toe. The most common variety. The extra digit may seem almost fully formed or may be attached only by a thin fleshy stalk. Typically an isolated finding. Common as a dominant trait in individuals of African descent. Managed by tying off with silk suture or transection of small skin tag. If involving bone, soft tissues, and tendons, referral to a hand surgeon is necessary.
Preaxial Polydactyly Next to 1st digit of hand or foot. Less common. Likely to be related to an underlying medical condition. Surgical correction is generally delayed for several months to lessen the risk of general anesthesia.
Clinodactyly • Slight medial incurvation of the fifth digit is a normal newborn finding. • Often inherited as a familial trait. • The absence of other physical findings confirms that it is benign and isolated.
Positional Deformity (Positional Calcaneovalgus) of the Foot Due to in utero positioning. Common foot deformity, especially in first-born. Hyperdorsiflexion of the foot with the abduction of the forefoot. The foot can easily be brought back to a neutral position. Resolves spontaneously, if not casting is indicated. PT that involves stretching and range of motion exercises can help speed progress.
Metatarsus Adductus • Most common congenital foot deformity. • Medial deviation (adduction) of the forefoot while hindfoot in normal position. • Forms a “C” shape. • More common in first-born. • Most common cause of in-toeing in infant. • 90% of cases resolve without intervention. • Tx: casting by 8 mo of age.