Download
1 / 29
290 likes | 397 Views
Name of Program. Medical Director’s Name and other team members. Overweight* Children in the U.S. (*BMI > 95th percentiles ). Source: NICHQ: JAMA, April 5, 2006, Vol 295, No. 13, 1549-1555. Did you know?. 1 out of every 3 children are overweight or obese

E N D
Name of Program Medical Director’s Name and other team members
Overweight* Children in the U.S. (*BMI > 95th percentiles) Source: NICHQ: JAMA, April 5, 2006, Vol 295, No. 13, 1549-1555.
Did you know? • 1 out of every 3 children are overweight or obese • Childhood obesity has more than doubled in the last three decades • $147 billion is spent on obesity every year • Children who are obese miss 4 times as many school days as non-obese children • Today’s children life expectancy may be less than that of their parents • In 10 years, the #1 reason for liver transplant will be from obesity, not hepatitis or cirrhosis
Cost and Health Impact of Childhood Obesity in Medicaid/SCHIP Enrollees From: Joe Thompson M.D. et al. Annual Silverman Lecture, Course number, 4600, Pediatric Academic Society, May, 2008 Arkansas Center for Health Improvement, Little Rock, AR; Pediatrics, University of Arkansas for Medical Sciences, Little Rock
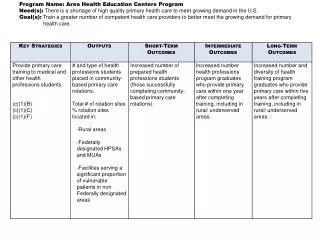
Desired outcomes for patients and families (one or more more) • Maintain or reduce BMI percentile • Slow down weight gain velocity • Improved co-morbidity measures (i.e. reduced blood pressure, reduced insulin levels, reduced fasting serum lipids) • Reduced medication usage • Increased school attendance • Improved emotional health
Multidisciplinary Obesity Care Team • Medical: MD,DO,APN • Nutrition: RD • Behavioral Therapy: PhD, MFT, LCMSW, MA • Physical Activity: PT, Exercise Physiologist • Care Coordination: RN, MSW, or Health Educator • Bariatric Surgeon (optional) Modified from: Barlow, S Expert committee Recommendations Regarding the Prevention, Assessment, and Treatment of Child and Adolescent Overweight and Obesity: Summary Report. Pediatrics, 2007.
Stages of childhood overweight treatment outlined by the AMA in 2007 and endorsed by AAP • Stage 1: Prevention Plus • Stage 2: Structured Weight Management • Stage 3: Comprehensive Multidisciplinary Intervention • Stage 4: Tertiary Care Intervention From: Barlow, S Expert committee Recommendations Regarding the Prevention, Assessment, and Treatment of Child and Adolescent Overweight and Obesity: Summary Report. Pediatrics, 2007.
Stage 1 Prevention Plus
Focus is on basic healthy lifestyle eating and activity habits • Minimize sugar-sweetened beverages with a goal of zero** • Increase meals prepared at home** • Education and modification of portion sizes** • Reduction of screen time to < 2 hours/day and if less than 2 years old to no screen time** • Increasing active time for children and families to >1 hour each day** • Involve the whole family in lifestyle changes • Cultural sensitivity ** = strong evidence
Focus is on basic healthy lifestyle eating and activity habits • Increasing to 5 fruit and vegetable servings or more per day* • Reduction of 100% fruit juices* • Consume a healthy breakfast* • Reduce foods that are high in energy density * • Meal frequency and snacking * • Involve the whole family in lifestyle changes • Cultural sensitivity *weaker evidence, but may be important for some individuals
Focus is on basic healthy lifestyle eating and activity habits • Eat Family meals 5-6 times per week • Involve the whole family in lifestyle changes • Allow child to self-regulate avoiding restrictive feeding behaviors. • Cultural sensitivity
After 3-6 Months • If Child has not made appropriate improvements move to Stage 2.
Management Decision Tree Adapted from: Spear BA, Barlow SE, Ervin C et al… Recommendations for Treatment of Child and Adolescent Overweight and Obesity. Pediatrics. 2007;120:S254-S288.
Management Decision Tree Adapted from: Spear BA, Barlow SE, Ervin C et al… Recommendations for Treatment of Child and Adolescent Overweight and Obesity. Pediatrics. 2007;120:S254-S288.
Management Decision Tree Adapted from: Spear BA, Barlow SE, Ervin C et al… Recommendations for Treatment of Child and Adolescent Overweight and Obesity. Pediatrics. 2007;120:S254-S288.
Stage 2: Structured Weight Management • Targeted behaviors the same as Prevention Plus, but more support and structure provided to the child to achieve these behaviors • Specific eating and activity goals with: • planned diet, structured daily meals and snacks • Supervised physical activity • Monitoring behaviors with logs • Additional reduction in inactive time • Planned reinforcement
Pilot Program for Stage 1 and Stage 2 Payment Plan • 4 Medical visits that may include other team members • 6 Dietitian visits • Review patient history following utilization of patient visits for reauthorization as needed Based on the Alliance for a Healthier Generations (Collaboration between the Clinton Foundation, AHA and 5 private health insurers: Aetna, BlueCross MA and NC, Pepsico, Wellpoint).
After 3-6 Months • If Child has not made appropriate improvements in Stage 2 move to Stage 3
Goals: To Support Tertiary Care Obesity Treatment • Improve access • Decrease disparity • Treat as a chronic medical issue • Extends medical home
Stage 3 Payment plan is based on building from Stage 1 Payment Plan* * Alliance for a Healthier Generations (Collaboration between the Clinton Foundation, AHA and 5 private health insurers: Aetna, BlueCross MA and NC, Pepsico, Wellpoint).
Stage 3 Comprehensive Multidisciplinary Intervention Payment Proposal
Stage 3 Comprehensive Multidisciplinary Intervention Payment Proposal
Next steps: • Prior Authorization Form filed with insurance plan.
In Conclusion • Childhood obesity affects both the physical and psychosocial health of children and may put them at risk of ill health as adults • Child and adolescent obesity has reached epidemic proportions and requires commensurate resources in prevention and treatment to change this trend

![[Insert Header/Program Name]](https://cdn0.slideserve.com/909144/slide1-dt.jpg)
![[Program Name] ORGANIZATIONAL CONFLICT OF INTEREST TRAINING](https://cdn1.slideserve.com/1565881/program-name-organizational-conflict-of-interest-training-dt.jpg)







![Program Baseline Assessment FY08 – 12 [Program Name]](https://cdn2.slideserve.com/4564931/slide1-dt.jpg)
![[name of home] Mentor Team Program](https://cdn2.slideserve.com/4749331/name-of-home-mentor-team-program-dt.jpg)
![[Program/Agency Name]](https://cdn3.slideserve.com/6646949/program-agency-name-dt.jpg)