Download
1 / 50
500 likes | 645 Views
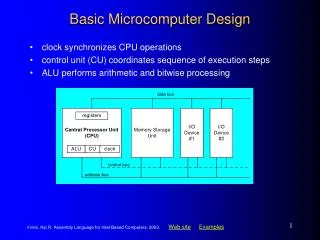
CPPT 9010: Facility Design & Operation. D.I.T. DT275 Masters in Chemical and Pharmaceutical Process Technology 8 th December 2009 Clement Farrar BA BAI MSc MIEI. Lecture Overview. 1) Quality & GMP 2) Regulatory Affairs 3) Safety & Environmental 4) Validation. 1) Quality & GMP.

E N D
CPPT 9010: Facility Design & Operation D.I.T. DT275 Masters in Chemical andPharmaceutical Process Technology 8th December 2009 Clement Farrar BA BAI MSc MIEI
Lecture Overview • 1) Quality & GMP • 2) Regulatory Affairs • 3) Safety & Environmental • 4) Validation
1) Quality & GMP Quality & Good Manufacturing Practice (GMP) • Where does it come from? • What is it? • What are the GMP Standards to be used? • Control mechanisms that assure Product Quality • What does it mean for day-to-day activities?
Quality ‘Quality is never an accident, it is always the result of high intention, sincere effort, intelligent direction and skilful execution; it represents the wise choice of many alternatives’ William A Foster
Quality & GMP - Where does it come from? • Patients taking medicines have very little chance of detecting anything wrong • If it is wrong, there is significant potential for a disastrous effect • They are complex products The patient has an implicit chain of trust!
Quality & GMP - Where does it come from? • As such, the manufacture of pharmaceuticals requires a special approach • We need both a Quality Assurance (QA) and a Good Manufacturing Practice (GMP) approach because: • Considerable limitations to drug product testing • Considerable risks from a low number of defectives • Low probability of detection (until too late) by the patient
GMP - What is it? GMP has been defined as: • The part of quality assurance which ensures that products are consistently produced and controlled in accordance with the quality standards appropriate to their intended use;
Quality Assurance - What is it? • Quality Assurance (QA) can be defined as: ‘The creation and operation of standards, procedures and management systems to guarantee the quality of a product throughout its life cycle.’ • These standards must be measurable, effective and relevant.
Quality Assurance - What is it? ‘Pharmaceutical quality assurance’ means the total sum of the organised arrangements made with the object of ensuring that medicinal products or investigational medicinal products are of the quality required for their intended use Ref: 2003/94/EC
Quality - What is it? • So, Quality Assurance is needed before, during and after manufacture along with systems for: • Complaints and adverse reactions • Recalls and returned goods • Market surveillance
Quality - What is it? • In respect to pharmaceuticals, quality can be describes as ‘fitness for purpose’ • It is the correct product • It is the correct strength or purity • It is free from contamination • It has not adversely deteriorated • It is correctly labelled and in the correct container • It is correctly stored
Quality Control (QC) • Facilities fit for intended use • Validated methods • Appropriate training systems • Samples of starting materials, intermediates, Drug Substance and Drug Product • Documented sampling and testing procedures
So, how does QA, GMP and product testing fit together to give us this assurance? Quality & GMP - What is it? Quality Assurance (QA) Good Manufacturing Practice (GMP) Quality Control (QC)
Control mechanisms that assure Product Quality • Documentation Systems • Validation • Change Control • Auditing and self inspection • Training • Calibration and Preventive Maintenance • Environmental control • Corrective Action Preventative Action (CAPA) • Quality Control Testing
GMP - What are the GMP Standards to be used? • EU Commission Directives • Legislative • EU Guide to Good Manufacturing Practice • Help in the interpretation of the legislation European legislation is directly concerned with the safety, quality and efficacy of medicines
Legislation/Guidelines • 2001/83/EC Community code relating to medicinal products for human use (QP and GMP Law) • 2003/94/EC Principles of GMP • EU - EudraLex - Volume 4 GMP Guidelines • Annex 1 – GMP for the Manufacture of Sterile Medicinal Products • Annex 2 - GMP for the Manufacture of Biological Medicinal Products for Human Use • FDA – CFR 210 &211
GMP - What are the GMP Standards to be used? • We have documented GMP Directives and Guidelines but there are clear expectations on the interpretation of these Directives and Guidelines • Similarly, through the mechanisms in the EU, these Guidelines are continually being reviewed in the light of these expectations hence current good manufacturing practice (cGMP)
GMP - What does it mean for day- to-day activities? • GMP helps you in that it gives guidance on: • The documents required • The responsibilities for their authorisation, control and completion • The responsibility for seeing that procedures are followed • How long any records should be retained for • What should be in the documents (SOP’s, batch records, etc.) How do you achieve this?
GMP - What does it mean for day-to-day Activities? • Ensure that you have the correct written procedures before starting the job – know what you are doing before you do it! • Ensure that you always work accurately and precisely – consistency and control • Ensure that the product is protected against contamination and mix-up • Ensure that the correct materials are being used • Ensure that all of those working with you have been appropriately trained to do the activities needed
GMP - What does it mean for day-to-day Activities? • Ensure that instructions are followed exactly and that all activities are appropriately documented and recorded • Ensure that everything is kept clean and tidy including you own personal hygiene • Ensure that there is an independent review of batch records prior to batch release by the Quality Unit • Ensure that all mistakes are reported immediately and learn from the errors (effective corrective actions implemented)
GMP - What does it mean for day-to-day Activities? So for you (Process Engineer?), what does GMP mean? • Simply, GMP is about the things you have to do, and the care each individual needs to take, on a day by day basis, to ensure the continued quality, safety and efficacy of your products. In this way, you can ensure the implicit chain of trust for the patient!
Quality/ GMP Guiding Principles • Quality systems are designed to meet all cGMP requirements specified under the US Code of Federal Regulations and equivalent EU Legislation • Facilities are designed to produce products meeting the highest quality standards to satisfy the needs of all its stakeholders through the application of the most up to date appropriate technologies and practices available • ‘Quality is everybody's business’ and the Quality Systems should support this principle to assure the start up of the facility in full compliance with all regulatory requirements while strengthening this quality culture among all contributors
When Quality Systems Fail • Inconsistent Manufacture • Contaminations • Rejected batches • Product defects • Recalls • Patient Safety
Exercise - The ‘F‘ Word • Review the extract • Count the number of times the letter ‘f’ appears within the extract, only carry out this count once How many f’s?
2) Regulatory Affairs • What is Regulatory Affairs? • Why do we need Regulatory Affairs • Regulatory Considerations • EMEA and FDA Organisations
What is Regulatory Affairs? • Protection of public health • Concerned with national and international framework of laws, regulations, guidelines and principles governing veterinary and human medicinal products • Rapid approval of new compounds emerging from the drug development pipeline • Interpretation of laws and regulations for project team members and management • Link between the Company and Regulatory Agencies
What is Regulatory Affairs? • All medicinal products must be approved before being marketed. EU directive 2001/83/EEC defines a medicinal product as: • Any substance or combination of substances presented for treating or preventing disease in human beings or animals • Any substance or combination of substances which may be administered to human beings or animals with a view to making a medical diagnosis or to restoring, correcting or modifying physiological function in human beings or animals is likewise considered a medicinal product
Why do we need Regulatory Affairs? • All medicinal products must be approved before being marketed. The Thalidomide tragedy of the 1960s revealed a new generation of synthetic drugs which were revolutionising medicine at the time but which also had the potential to harm as well as heal. • Thalidomide, approved in Europe in 1957, was developed as a sedative and anti-anxiety medication • No teratogenicity (the ability to cause birth defects) studies had been carried out, at that time the use of drugs in pregnancy was not well documented and Thalidomide was widely prescribed during pregnancy • Wiedeman described the syndrome of phocomelia (seal like limbs) in 1961, with 13 case histories presented. The connection with Thalidomide was realised later that year, 1 in 3 women exposed to the drug in the third trimester had affected infants • Thalidomide was removed from the market in 1961, by which time more than 10,000 infants had been born with malformations
Regulatory Considerations Regulatory Compliance & Design Implications For Multi-Product Facilities (Worst Case Scenario)
Regulatory - Multi Use Facilities Considerations • Multiple products in facility • Multiple lots at various stages in facility • Campaigning multiple products • Similar products • Different products
Regulatory - Risks of Multi-Use Facilities • Contaminants are introduced that are difficult to detect • Cross-contamination between products • Product carryover • Operators working in multiple product areas • Preparation of ‘unknown’ materials within the production facility Consider: – Contract Manufacturing Organizations (CMOs)
Regulatory - Risks of Multi-Use Facilities FDA - Primary Concerns: • Cross contamination - Generation of aerosols (spills, equipment leakage) - Campaigning within the same area - Concurrent production • Potential for mix-ups and microbial contamination - Inadequate segregation - restricted access - Open processing - air quality/ monitoring • Lack of facility controls - Area clearance/ cleaning/ inactivation - Personnel training/ qualification - Good documentation practices - Utilities
Regulatory - Multi-Use Facility Design • Design must allow for: – Adequate separation of manufacturing activities – Proper flow of materials and product – Appropriate level of containment, and movement of personnel within the facility • Facility must have: – Good plant support systems [systems that could affect the SISPQ (Strength, Identity, Safety, Purity, or Quality) of the manufactured product]: - (HVAC, Water, Steam, CIP, and Waste) – Validation program: - Equipment, Cleaning, Changeover
Regulatory - Multi-Use Facility Design • Design must have (continued): – Good calibration and preventive maintenance programs – Good environmental monitoring programs to routinely verify the quality of air and water – Good personnel training program: - Current Good Manufacturing Practices (cGMPs) - Necessary skills and techniques to perform their assigned functions - Awareness of the unique properties of biological products and their potential impact on a manufacturing process (if applicable)
Regulatory - Logistics Design • Sufficient space for equipment and processes • Separate or well defined areas for manufacturing processes – Time (procedural) – Space (separate, dedicated areas) – Air system control (containment areas) • Flow patterns – Two corridor system – Single corridor system – Air system control (containment areas) • Adequate storage available for clean and dirty equipment and in-process materials
Regulatory - Material Flow Design • Suitable areas for quarantine/ release – Raw materials and components – In-Process intermediates – Bulk material [Active Pharmaceutical Ingredient (API)] – Final product • Logical flow through facility • Hard piped vs. transport
Regulatory - Personnel Flow Design • Restricted access • Adequate gowning areas/ levels • Segregation of different functions – Glassware washing, production, filling operations
Regulatory - Equipment Considerations • Class/Type: disposable, dedicated, shared • Dedicated: – Properly identified, labelled, stored – Adequate maintenance and calibration – Documented use (logs) • Shared: – Appropriately design for >1 product/host – Easily cleaned and sterilized – Properly identified as to use and status – Rigorous maintenance and calibration programs – Documented use (logs) and changeover procedures
Regulatory - Equipment Flow • Adequate segregation of clean/ dirty equipment • Appropriate areas for decontamination and cleaning • Adequate areas for storage of equipment when not in use
Regulatory - Sterilization Systems • Facilities should be provided with adequate sterilization systems for containment and aseptic processing areas • Autoclaves for moist heat sterilization • Dry-heat ovens for depyrogenation • Use of double doors for appropriate materials flow • Separate systems for decontamination recommended • Sterilized materials should ‘cool-down’ under controlled air • Validation studies should include: – Empty chamber studies – Representative loads – Challenge studies, as appropriate
Regulatory - Changeover Procedures • Removal of all product, process materials and disposable equipment from processing area • Equipment that is dedicated to a single product is adequately identified, cleaned and removed from processing area to a controlled storage area • All non-dedicated equipment that remain in the processing area are cleaned using validated cleaning agents. Protective covering during non-use • A close out inventory (checklist) is conducted to assure that all materials, documents, equipment and SOPs have been properly attended to and completed. • Processing areas approved for the next product campaign by the quality department
EMEA & FDA EMEA and FDA Organisations
EMEA - European Medicines Agency • Decentralised body of the European Union with the headquarters in London • Established in 1995 • Main responsibility is the protection and promotion of public and animal health through the evaluation and supervision of medicines for human and veterinary use • Governing body is European Commission
FDA Mission • The FDA is responsible for protecting the public health by assuring the safety, efficacy, and security of human and veterinary drugs, biological products, medical devices, our nation’s food supply, cosmetics, and products that emit radiation. The FDA is also responsible for advancing the public health by helping to speed innovations that make medicines and foods more effective, safer, and more affordable; and helping the public get the accurate, science-based information they need to use medicines and foods to improve their health. • Established in 1906
Key Differences between FDA and EMEA Inspections • The EU cGMP guidelines tell you what is required, not how to do it, while the FDA guidelines focus more on how to achieve various standards. • This is the key difficulty in the negotiations ongoing between the EU and the FDA on mutual recognition of manufacturing inspections. • The EU cGMP guidelines do recognise that there are acceptable alternative methods for achieving the same objectives.
Key Differences between FDA and EMEA Inspections • FDA Investigators look for compliance with cGMP regulations and fundamentally are looking for violations of these regulations • With the EMEA there may be substantial dialogue on technical issues between the management of a facility and the EU inspectors, however, the FDA approach is more ‘gung ho’ and adversarial. • FDA inspections can last for months, whereas the EU inspections are typically for several days to a week maximum • Further evidence of the more adversarial role of the FDA is evidenced by the fact that many companies have legal staff present during an FDA audit, with FDA auditors even accompanied to the toilets!
Key Differences between FDA and EMEA Inspections • The FDA inspections tend to be paper-based, with a review of all relevant records and procedures, while the EU auditors can tend to spend more time visiting the site and inspecting the relevant utilities, equipment and performance of personnel. • The FDA tend to be ‘black and white’, while the EU inspectors will show more leeway and take a more ‘holistic’ approach to the organisation that they are inspecting. • Indeed, the European commission working party on the control of medicines and inspections wrote in 1995 that ‘the task of an inspector is not limited to the disclosure of faults, deficiencies and discrepancies. The inspection should connect an observation with assistance in making the necessary improvements. An inspection should normally include educational and motivating elements.’
FDA Basic Inspection Techniques - similar to EMEA • Observation • Conditions, Behaviour, Document • Tours/walkthroughs • The majority of problems are identified/’hinted at’ during the tour. • Inspectors look for ‘predictors’ and look for the ‘impact’ of a particular issue elsewhere • Inquiry • Document review • Compare and confirm • Samples are taken – if they see a problem
Some Key Acronyms and Definitions • FDA-483: A list of adverse observations issued at the end of an inspection • FDA Warning letter: Depending upon the severity of the findings, the company may receive an FDA Warning Letter summarizing the finding of the inspection • Consent Decree: If a firm has repeatedly violated cGMP requirements and have not addressed the FDA 483 Inspection Observations and Warning letters, the FDA may make a legal agreement with the firm to force them to make specific changes; the agreement, the Consent Decree, is enforced by the federal courts. Increasing severity