Download
1 / 42
420 likes | 614 Views
“Adjunctive Therapy” Non ST segment elevation ACS. Dr M R Thomas King’s College Hospital. Advanced Angioplasty 2002. Plaque Rupture. Unstable angina. Non ST elevation AMI. ST elevation AMI. “Adjunctive Therapy” Non ST segment elevation ACS. Pre-PCI (assume DGH admission) Peri-PCI

E N D
“Adjunctive Therapy”Non ST segment elevation ACS Dr M R Thomas King’s College Hospital. Advanced Angioplasty 2002
Plaque Rupture Unstable angina Non ST elevation AMI ST elevation AMI
“Adjunctive Therapy”Non ST segment elevation ACS • Pre-PCI (assume DGH admission) • Peri-PCI • Post PCI UK Perspective!!
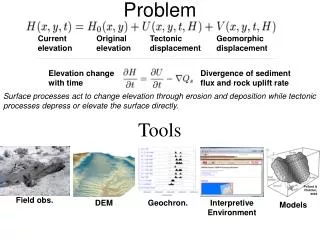
“Adjunctive Therapy”Non ST segment elevation ACSPre PCI • Obvious medical therapy. • - aspirin. • - anti-anginals. • - lipid lowering. • MIRACL: • 80mg atorvastatin v placebo • Un angina/non Q MI • Rx for 16 weeks • Primary endpoint: death, non fatal MI,cardiac arrest and emergency re-hospitalisation P=0.048 MIRACL TRIAL
Is there a need for revascularisation? • And therefore generally transfer to a tertiary centre.
High surgical mortality. 7.7% overall and 12% in the invasive arm
Median time to angiography 4 days Median time to revascularisation 4 (PCI) to 7 (CABG)
Median time to angiography 22 hrs Median time to revasc 25 (PCI) to 89 (CABG) hrs
“Adjunctive Therapy”Non ST segment elevation ACSSo assuming some or all patients will need revasularisation (PCI) what is the best type and combination of drugs pre PCI • Heparin, UFH or LMWH • IIb/IIIa receptor inhibitors • Clopidogrel
Heparin: LMWH or UFH • Essence and TIMI 11B • These trials have demonstrated an advantage of LMWH over UFH in UA and other trials have shown at least equivalence. • Also ease of use compared to UFH. • Worries about combination • with IIb/IIIa now resolved.
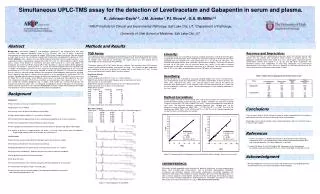
Incidence of death/MI in patients at 1 year: effects of enoxaparin more marked in PCI patients, TIMI 11B/ESSENCE meta-analysis OR (95% CI) 0.61 (0.35,1.06) OR (95% CI) 0.72(0.49,1.04) OR (95% CI) 0.92(0.81,1.04)
IIb/IIIa receptor inhibitors • “National Institute of Clinical Excellence” • Guidance on the use of glycoprotein IIb/IIIa inhibitors in the treatment of acute coronary syndromes. September 2000 • (1) For high risk patients with unstable angina or non-Q MI, the intravenous use of GP IIb/IIIa inhibitors in addition to low (adjusted) dose UFH is recommended. • (2) In unstable angina, raised blood levels of troponin should be used to identify those at high risk. NB: Pre GUSTO IV ACS
In the absence of revascularisation value of IIb/IIIa receptor inhibitors “small” and evidence favours small molecules.
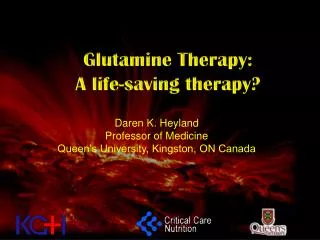
CURE CURE (OASIS-4) Clopidogrel in Unstable Angina to prevent Recurrent ischemic Events
Placebo Cumulative Hazard Rates Clopidogrel P < 0.001 0 3 6 9 12 No of Pts Months of Follow-up Plac Clop 6303 6259 5780 5866 4664 4779 3600 3644 2388 2418 Cumulative Hazard Rates for CV Death/MI/Stroke 20% RR cp 20% Prism + 6/12 9.6% Pursuit 30 days 11.4% 9.3%
Transfer for revascularisation. • Does everyone need to be transferred for angiography and possible revascularisation?
Risk stratification Baseline ST segment change Recurrent Ischaemia
Prognostic value of Baseline Troponins Gusto IIA: 30 day mortality (%) P<0.001
TACTICS-TIMI 18: Stratified by Troponin T OR=0.47 p=0.002 OR=0.95 p=NS
Low risk patients • Data supports an ischaemia-guided approach with treadmill exercise or pharmacological stress.
Transfer! • So we have transferred the high risk patient: • - troponin +, recurrent ischaemia, ST depression. • ON • - aspirin, LMWH, clopidogrel, IIb/IIIa in ideal world!! (24 hrs) • BUT • in UK aspirin, LMWH and clopidogrel (2 weeks!)
Transfer • Is there a problem with LMWH and IIb/IIIa?
“Acute II” • First randomised trial of IIb/IIIa blockers and LMWH in ACS. • 525 ACS patients on aspirin and Tirofiban (Aggrastat). • Randomised to LMWH (enoxaparin) or UFH. • Primary endpoint: SAFETY.
30 day event rates in ACUTE II Paragon-B appears to similar results for Lamifiban
International Task ForceRecommendations (Feb 2001)(Karl Karsch from UK)
IIb/IIIa receptor inhibitors • Which patients…….all or defined by coronary anatomy? • Which compound………?any • Delivered when………?upstream or after diagnostic angiogram.
“Adjunctive Therapy”Non ST segment elevation ACSPost Discharge • 2ary prevention, lipids etc • Aspirin • Clopidogrel
PCI- A prospective, randomized, double-blind substudy of patients undergoing PCI in the CURE trial
0.08 Placebo 0.06 Cumulative Hazard Rate 0.04 Clopidogrel RR 0.70 95% CI 0.50-0.97 P=0.03 0.02 0.0 5 10 15 20 25 30 Days following PCI Primary Endpoint:CV Death, MI, Urgent Revascularization Mehta SR et al. Lancet 2001:358:527-33
Placebo 0.10 0.08 0.06 Cumulative Hazard Rate Clopidogrel 0.04 RR 0.75 95% CI 0.56-1.00 P=0.047 0.02 0.0 0 100 200 300 400 Days following PCI CV Death, MI:From PCI to End of Followup Mehta SR et al. Lancet 2001:358:527-33
CV Death or MI at Various Intervals RRR 31% 32% 34% 21% * *P=0.002 Mehta SR et al. Lancet 2001:358:527-33
Guidelines • “Guidelines for the management of patients with acute coronary syndromes without persistent ECG ST elevation” • Heart 2001;85:133-142
We live in the UKQuestions • Where should diagnostic angiography be performed? • Where should interventional cardiology be performed? • Who should perform interventional procedures? • How do we increase the availability of both of the above? • ALL OF THE ABOVE IS AS/MORE IMPORTANT AS THE DATA!
Conclusions • I think we know the data: • aspirin, lipid lowering, clopidogrel, LMWH, risk assessment and IIb/IIIa with early revascularisation in the high risk group. • Providing an optimal service in the UK via the NHS…….now that’s a different story!!