Download
1 / 30
320 likes | 584 Views
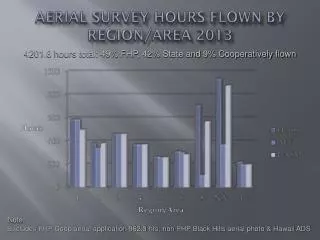
Force Health Protection (FHP) Brief for the NAVAF AOR. Preventive Medicine CNA-C6F Medical. In general: Poor Rural Poor Health Infrastructure. Force Health Protection Guidance. INTERIM FLEET GUIDANCE FOR DEPLOYMENTS TO AFRICA, CFFC 221531 JUL 11

E N D
Force Health Protection (FHP) Brief for the NAVAF AOR Preventive Medicine CNA-C6F Medical UNCLASSIFIED
In general: • Poor • Rural • Poor Health • Infrastructure UNCLASSIFIED
Force Health Protection Guidance • INTERIM FLEET GUIDANCE FOR DEPLOYMENTS TO AFRICA, CFFC 221531 JUL 11 • FLEET FORCE HEALTH PROTECTION GUIDANCE FOR DEPLOYMENTS TO AFRICA, C6F 141113Z May 10: • FHP is a Commander's responsibility and shall be aggressively supported by your Medical Departments • COMSIXTH FLEET Surgeon pushes “Smart Packs” containing specific FHP guidance and medical operational guidance to all C6F in bound units 30-45 days before inchop. • Centers for Disease Control, Traveler’s Health information: wwwnc.cdc.gov/travel/destinations/list.aspx • National Center for Medical Intelligence: www.ncmi.dia.smil.mil/index.php UNCLASSIFIED
Force Health Protection Guidance • To prevent disease and non-battle injuries (DNBI) Commanders will: • institute effective FHP measures and • health surveillance/reporting and • take action to reduce health hazards • Programs integral to pre-, during and post- travel/deployment • Ensure strict compliance with • pre-travel medical screening requirements • post-deployment health assessments if required UNCLASSIFIED
Pre-Travel Activities • Medical screening • HIV, PPD, G6PD results in health record • All appropriate DoD and country specific requirements for immunizations • Anti-malarial medication prescribed, if needed • Uniforms and civilian clothes for travel pre-treated with permethrin • Issued permethrin-treated bednet • Issued 30% DEET insect-repellant lotion UNCLASSIFIED
Travel to Africa Health Risks Water and food-borne illnesses Vector-borne diseases Heat injury Rabies and other animal diseases Motor vehicle crashes UNCLASSIFIED
Diseases of Operational Significance • Food & Waterborne Diseases • Diarrheal diseases and hepatitis A • Sanitation variable but well below US standards • Sewage contaminates surface water sources • Variety of bacteria, viruses, and parasites present UNCLASSIFIED
Diseases of Operational Significance • Food & Waterborne Diseases • Prevention • Wash hands frequently • Avoid street vendors/stalls • Eat at nice international chain hotels and Embassy recommended restaurants • Avoid raw foods unless you peel them yourself—no lettuce/salads • Avoid buffets where food sits out at room temperature • Only drink treated water from approved sources or drinks with tops you remove yourself • Avoid ice – freezing does not kill the bacteria/viruses • Cook it well, peel it or don’t eat it! UNCLASSIFIED
Textbook of Travel Medicine UNCLASSIFIED
Prevention ofDiseases Spread by Food & Water • HAND WASHING • After bathroom, before meals • Use hand sanitizer when hand washing not possible UNCLASSIFIED
Insect Vectors UNCLASSIFIED
Diseases of Operational Significance • Vector-borne diseases widespread in Africa • Vectors include mosquitoes, sandflies, ticks, lice, flies and fleas. • Risk to US forces of: • Malaria, yellow fever, dengue, plague, tick-borne encephalitis, typhus, lassa fever, Crimean-Congo hemorrhagic fever, sandfly and West Nile fevers, relapsing fever, filariasis, tungiasis, leishmaniasis, loiasis, trypanosomiasis, and onchocerciasis. • These diseases can significantly impact force health unless preventive measures are enforced. • Prevention of insect/arthropod bites (24 hrs/day) is key, especially as some vector-borne diseases have no specific treatment available. UNCLASSIFIED
MALARIA • Malaria can be rapidly fatal; take all available measures to prevent the disease. Preventive medication is required but not sufficient. • Malaria prevention is required for travelers to all African countries except Algeria, Egypt, Lesotho, Libya, Mauritius, Morocco, Seychelles, and Tunisia. • Swaziland, Cape Verde, and South Africa have limited areas of risk. • While Plasmodium falciparum, vivax, ovale, and malariae strains may all be encountered in Africa, falciparum is the most widespread, serious, and most commonly fatal type of malaria. • The malaria parasite is spread by the bite of the Anopheles mosquito UNCLASSIFIED
MALARIA • Clinical Aspects • Incubation period about 10 days after an infective mosquito bite – if you become sick after about a week in Africa, seek medical attention • Usually starts as mild fever illness with nonspecific symptoms: • Fever, and/or headache, malaise, chills, sweats, cough, diarrhea, • Always a possibility in sick person with potential exposure — • any fever in country with malaria could be malaria until proven otherwise UNCLASSIFIED
MALARIA • Prevention • Prevention of vector borne diseases including malaria: • Personal protective measures • Permethrin-treated clothing worn properly • DEET lotion on skin not covered by clothing • Sleep under permethrin-treated bednet • Preventive medication (chemoprophylaxis) • Preventive medication “should be viewed as the last arm of a comprehensive anti-malarial program - a final barrier to illness after barriers of DEET, permethrin-treated uniforms and bednets have been employed. Like conduct ashore, this is a leadership issue.” • Shipboard personnel in port and outside the skin of the ship are equally at risk as those ashore. UNCLASSIFIED
Plus permethrin-treated civilian clothing; long sleeves/pants of at least 50% cotton material UNCLASSIFIED
Vector Avoidance ‘Pop-up’ permethrin-impregnated bednets Approved 30% DEET repellant lotion Bulk permethrin spraying of uniforms IDA “shake and bake” permethrin kit UNCLASSIFIED Aerosol permethrin spray
MALARIA • Malaria Prophylaxis Medications • Drug choice depends on various factors including length of travel, destination, allergies and medication history, etc. • Recommend Malarone, with mefloquine or doxycycline as other options • Malarone (250mg/100mg) 1 tablet daily, start 1-2 days before entry • Mefloquine (250 mg) 1 tablet weekly, start 2-3 weeks prior to entry in country • Doxycycline (100 mg) 1 tablet daily start 1-2 days before entry • After leaving country: • continue Malarone for 1 week, or mefloquine or doxycycline for 4 weeks • Plus, may need to add primaquine daily for 14 days if G6PD test normal and indicated by region/duration of travel UNCLASSIFIED
MALARIA • Personnel must be medically screened and malaria chemoprophylaxis individually prescribed. • Directly observed therapy (DOT) is mandatory for all anti-malaria drug regimens to ensure compliance. • Chain of command support is required to carry out DOT, with supervisory personnel observing members take daily or weekly medication, keeping a daily log, and keeping log on file for 3 months after return. • Qualified medical personnel must brief all deployers on country-specific health threats and relevant countermeasures. UNCLASSIFIED
MALARIA PREVENTION SUMMARY • COMMANDERS SHALL ENSURE THAT ALL PERSONNEL ARE PREPARED WITH THE FOLLOWING SET OF PERSONAL PROTECTIVE EQUIPMENT (PPE): • TWO SETS PERMETHRIN TREATED UNIFORMS (E.G. NWU, BDU, OR DCU) • TWO SETS PERMETHRIN TREATED CIVILIAN CLOTHES (LONG SLEEVED SHIRTS AND LONG PANTS) FOR TRAVEL AND LIBERTY • ADEQUATE SUPPLY OF DOD-ISSUED DEET INSECT REPELLENT LOTION • A PERMETHRIN TREATED BEDNET • MALARIA PREVENTIVE MEDICATION PRESCRIBED, SUPPLIED, AND TAKEN AS MEDICALLY DIRECTED. UNCLASSIFIED
Two of Many Other Diseases Spread by Insects leishmaniasis myiasis UNCLASSIFIED
Other Diseases of Operational Significance • Water Contact Diseases • Leptospirosis • Freshwater contaminated by animal urine • Schistosomiasis • Freshwater contaminated by urine/feces of infected person • Prevention • Avoid swimming in fresh water--lakes, rivers/streams • Rinse and vigorous toweling after unavoidableexposure UNCLASSIFIED
Other Diseases of Operational Significance • Sexually Transmitted Diseases • HIV • Hepatitis B & C • All others—gonorrhea, syphilis, etc. • STDs very common particularly among commercial sex workers (up to 80% infected) UNCLASSIFIED
Force Health Protection Guidance • Climate • Heat injuries can be greatest overall threat during travel to warm climates • Acclimatization takes 10-14 days. • Proper work-rest cycles, adequate hydration, command emphasis on heat injury prevention • Awareness that illness, sunburn, drinking alcohol, older age, poor physical condition, certain drugs increase vulnerability to heat. UNCLASSIFIED
Force Health Protection Guidance • Animal Avoidance. • Very poisonous snakes are found throughout Africa • common in rural/field settings • most snakes will flee from humans • educate personnel on snakebite prevention • Don’t play with snakes • Move slowly through brush/scrub • Beware reaching under piles of rocks, wood, etc. • Antivenoms • Due to specificity, poor shelf life, and general lack of availability, not practical to deploy with antivenom onboard. • US Embassy has local information regarding suitability and availability of antivenom. • Street/wild dogs carry rabies, leishmaniasis, herpes B virus, and tickborne encephalitis. • Avoid any contact with local animals, report urgently for treatment of any bites or scratches. • Dog with rabies may appear calm – not always snarling/foaming at the mouth UNCLASSIFIED
Force Health Protection Guidance • Automobile accidents • Number One cause of non-combat death in military personnel traveling overseas • Road conditions very poor • Drivers often untrained/erratic • Always wear seatbelt • Drive defensively • Avoid driving at night UNCLASSIFIED
Medical Emergency Contacts • - C6FBattle Watch Officer: COM 011-39-081-568-4551/4552 • - TRICARE International SOS (ISOS):011-44-20-8762-8133 e-mail: tricarelon@internationalsos.com • - USNH Rota, Spain:COM or 011-34-956-82-3305 • - USNH Naples, Italy:COM: 011-39-081-811-6192/6155 • - USNH Sigonella, Italy:COM: 011-39-095-56-3842 • - US Army Regional Medical Center Landstuhl, Germany:COM: 011-49-6371-86-8106 • - Theater Patient Movement Requirements Center (TPMRC) Europe:STU-III Capable DSN 314-480-8041/42 or COM 011-49-63-7147-2264/8042 UNCLASSIFIED
Post-Deployment/travel Activities • Post-deployment Health Assessment questionnaire if required (after deployments of 30 days or more) • Complete all malaria medications as instructed • See health care provider immediately for any fever or unexplained/persistent symptoms (diarrhea, cough, rash, etc.) UNCLASSIFIED
Contact Information For country-specific guidance and travel medicine recommendations contact: • NEPMU-2, Norfolk VA, DSN 377-6600 NEPMU2NorfolkThreatAssessment@med.navy.mil • Local MTF • NAVAF Medical, DSN 626-4690/6204 or cne-c6f_hss@eu.navy.mil • Centers for Disease Control, Traveler’s Health information: wwwnc.cdc.gov/travel/destinations/list.aspx UNCLASSIFIED