Download
1 / 24
240 likes | 250 Views
Cancer Pathology Electronic Reporting Standards: New NAACCR Volume V- with Specimen Information. Jovanka N. Harrison, PhD Chair, NAACCR Pathology Data Work Group Research Scientist, New York State Cancer Registry NAACCR Annual Conference Québec City, Canada June 22, 2010. Outline.

E N D
Cancer Pathology Electronic Reporting Standards:New NAACCR Volume V- with Specimen Information Jovanka N. Harrison, PhD Chair, NAACCR Pathology Data Work Group Research Scientist, New York State Cancer Registry NAACCR Annual Conference Québec City, Canada June 22, 2010
Outline NAACCR Path Data Work Group History of NAACCR E-Path Standards Introduction to HL7 NAACCR Volume V, Version 3.0 (July,’09) Conformance Testing Tools NAACCR Path Data Work in Progress
NAACCR Pathology Data WG 2009-2010 A Collaboration between Canada and the U.S. Jovanka Harrison, PhD (Chair)Elaine Hamlyn, HRT, CTR Robin Rossi New York State Cancer Registry CPAC Cancer Care Ontario Mayra Alvarez, RHIT, CTRLori A. Havener, CTRMark Rudolph Florida Cancer Data Systems NAACCR, Inc. Florida Cancer Data Systems Victor Brunka Mary Kennedy, CT, MPHWendy Scharber, RHIT, CTR AIM SNOMED International Registry Widgets Kathleen Davidson-Allen, CTRCarol Kosary, MS Beth Schmidt, MSPH Northern Calif. Cancer Center NCI SEER Louisiana Tumor Registry Eric B. Durbin, MSKeith Laubham, MD Kentucky Cancer Registry Arizona Cancer Registry Advisors to the WG: Ted Klein Ken Gerlach, MPH, CTRAndrea MacLean Klein Consulting CDC/NPCR CPAC Austin Kreisler Barry Gordon, PhDVarun Mediratta SAIC C/Net Solutions Cancer Care Ontario Catherine Grafel-AndersonRichard Moldwin, MD, PhD Hawaii Tumor Registry SNOMED International
NAACCR Path Data WG- Cont’d Goal: “Develop messaging standards for transmission of electronic reports from anatomic pathology laboratories to cancer registries” Overall Aims: improve efficiency, reduce cost and provide a structure for future E-path initiatives
History of NAACCR E-path Standards 2000 – First version- Chapter Six in Vol. II 2005- Second version- Volume V 2008- Volume V, Version 2.1 (HL7 v.2.3.1) February 2009- Volume V, Version 2.2 July 2009- Volume V, Version 3.0 (HL7v.2.5.1) July 2010 – In progress, Volume V- synoptic reporting, including College of American Pathologists electronic Cancer Checklists
History of NAACCR E-path Standards Cont’d Volume V, Version 3 (July, ‘09) defines the standard using HL7 v. 2.5.1-with corresponding Implementation Profiles Why the HL7 v.2.5.1? HL7 Version 2.3.1 is no longer actively supported by HL7. Standard HL7 v. 2.5.1 allows for more robust ways of transmitting specimen information (the SPM segment)
Introduction to HL7 - Part 1 An HL7 2.xmessage*is comprisedof agroup ofsegments ordered in a hierarchical and defined sequence. Segmentscontain logicalgroupings ofdata fields Data fields may contain one or more components Components may have one or more sub-components *Unit of data transferred between systems in a single transmission
Introduction to HL7- Part 2 Data fields are separated by a field separator or delimiter Usually a “pipe” character (|) If a field has several components, they are separated by a “hat” character (^) If a component has sub-components they are separated by an (&) Segmentscan be required, optional, or allowed to be repeated Brackets around Segments indicate: [ ] an optional segment { } a segment which can be repeated [{ }] an optional segment which can be repeated
Introduction to HL7- Part 3 How do we know if a message is conformant/compliant to a specific HL7 standard? Standard conformance may be documented in any of the three basic profile types: HL7 Standard Profile (i.e., published standard) Constrainable profile (“Optional”) Implementation profile (no ‘optional parts’, ready to be implemented)
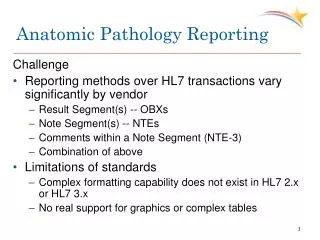
NAACCR Volume V, Version 3.0 Focus on transmission of traditional text-based pathology reports with emphasis on specimen information (HL7 v. 2.5.1) TheUse Case Story Board (Process Flow Diagram) and the Dynamic Interaction Model (UML activity diagram) (Section 2.3.2) show three scenarios: 1) Single reporting source with multiple specimens 2) Service model- use of a reference lab for accessioning of specimens 3) Service model with a consult
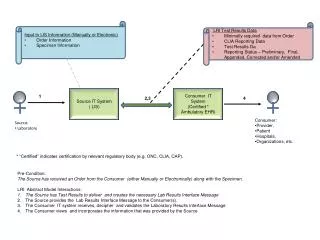
Example- A Simple Use Case Model* * Adapted from NAACCR Volume V, Version 3, Chapter 2, p.10
Example- Section of A Process Flow Diagram* Central Cancer Registry Surgery Path Lab LIS Pathologist * Adapted from NAACCR Volume V, Version 3, Chapter 2, p.13
Example- Part of an UML Activity Diagram* * Adapted from NAACCR Volume V, Version 3, Chapter 2, page 14
NAACCR Vol. V, Version 3.0 Cont’d Sample HL7 messages provided for: 1) A “Simple Case”- a single reporting source, single primary with multiple specimens 2) A “Complex Case”- multiple: primaries specimens types of reports
“Simple Case”- HL7 v. 2.5.1 Example (modified)NAACCR Volume V, Version 3.0 Note: Single reporting source and single primary; two specimens MSH|^~\&|ILS|Indep Lab Services-NY^33D1234567^CLIA|ECLRS|…<CR> PID|1||123456789^^^^SS|000039^^^^LR|McMuffin^Candy^^^Ms.|…<CR> PV1|N|||||594110NY^Attending^Doctor^^^DR|…<CR> ORC|RE||||||||||||||||||||Albany Medical Center^^123456^^^AHA|2 Canada Ave|…<CR> OBR|1||97865|11529-5^SURG PATH REPORT^LN^^PATH REPORT^L|…<CR> OBX|1|TX|22636-5^CLIN HISTORY^LN|| …white F with (L) UOQ breast mass|…<CR> OBX|2|TX|22638-1^COMMENTS^LN||Carcinoma of breast. Post op dx same.|…<CR> SPM|1|^97865-1&ILSPCID||TISS^Tissue^HL70487|||||||||||||200407200930|…<CR> OBX|3|TX|22633-2^Nature of Spec^LN^L47^Submitted Tiss^L|1| L breast biopsy|…<CR> OBX|4|TX|22634-0^Gross Path^LN^L567^Gross Path^L|1| #1 received fresh…|…<CR> OBX|5|TX|22637-3^Path report final dx^LN|1|1.Infiltrating duct ca, left breast.|…<CR> SPM|2|^97865-2&ILSPCID||TISS^Tissue^HL70487|||||||||||||200407200930|…<CR> OBX|6|TX|22633-2^Nature of Spec^LN^L47^Submitted Tiss^L|2| L radical mastect|…<CR> OBX|7|TX|22634-0^Gross Path^LN^L567^Gross Path^L|2|#2 cont of L rad mastec|…<CR> OBX|8|TX|22637-3^Path report final dx^LN|2|2. Metastatic breast carcinoma..|…<C>
Note: Three OBR segments included: 1)Summary report,2) path text reportand3) synoptic report*– all for one patient OBR|1||S91-1700|11529-5^SURG PATHREPORT^LN^^PATH REPORT^L|…<CR> OBX|1|TX|^^^L117^CASE REVIEW^L|1|Case reviewed ..M.D. resident…|<CR> OBX|2|CE|21988-1^Site ICD-O-1^LN|2|C679^Bladder wall^ICDO3|…<CR> OBX|3|CE|21988-1^Site ICD-O-1^LN|3|C187^Sigmoid colon^ICDO3|…<CR> etc. OBR|2||S91-1743|^^^L25^TEXT PATHREPORT^L|…<CR> SPM|1|^92756A&HITECSPCID||TISS^Tissue^HL70487|||||||||||||200704020930|…<CR> OBX|13|TX|^^^L47^Submitted Tiss^L|4| A (fsi) (gums) Bladder tumor|…<CR> OBX|14|TX|^^^L567^Gross Path^L|4|Please see description in Inter Op Consult|…<CR> OBX|15|TX|22637-3^Path report final dx^LN|4|Bladder tumor, inv urothel carc|…<CR> etc. SPM|8|^92756H&ILSPCID||TISS^Tissue^HL70487|||||||||||||200407200930|…<CR> OBX|46|TX|^^^L47^Submitted Tiss^L|11| H (gurs) Rectum|…<CR> OBX|47|TX|^^^L567^Gross Path^L|11| Specimen consists of sig colon, rectum..|…<CR> etc. OBX|49|TX|22637-3^Path report final dx^LN|11|Adenoca of the colon...|…<CR> “Complex Case” - HL7 v. 2.5.1 Example (modified)NAACCR Volume V, Version 3.0 *The synoptic report section is not shown here– the 3rd OBR is followed by a number of OBXs (OBX-3 and OBX-5 pairs indicating question and answer sections from a specific CAP checklist.
Conformance Testing Tools HL7 Messaging Work Bench (MWB) Free-ware for validating conformance of HL7 (2.x) messages Developed by Peter Rontey (initially for the VHA system) NAACCR Implementable Conformance Profile for Volume V, Version 3 available at the NAACCR web site http://new.naaccr.org/StandardsandRegistryOperations/VolumeV.aspx
Conformance Testing Tools Cont’d The HAPI Parser- open source HL7 2.x parser for Java User-friendly Perfect for testing of short (demo-type) messages Recently updated (May 15, 2010) Initiated by University Health Network Large multi-site teaching hospital in Toronto, Canada http://hl7api.sourceforge.net/
Conformance Testing Tools Cont’d. Electronic Mapping, Reporting and Coding Plus (eMaRC Plus) Developed by Centers for Disease Control and Prevention CDC/NPCR-AERRO and programmed by their Registry Plus Development Team (S. Baral) HL7 files manually imported then parsed Mapping to NAACCR data elements NAACCR style abstract records available for review by Certified Tumor Registrars Uses NegEx algorithm to differentiate between reportable and non-reportable terms Next release: parsing an HL7 2.5.1 message http://www.cdc.gov/cancer/npcr/tools/registryplus/mp.htm
Work in Progress:Synoptic Reporting The NAACCR Pathology Data WG and its special work group “NAACCR Path Data CAP Checklist WG” is enhancing Volume V, Chapter 3: Synoptic Reporting Using the CAP electronic Cancer Checklists (eCC). Guidelines and examples Transmission of path reports in the CAP eCC format for selected cancer sites: breast (invasive and DCIS), prostate, colorectal, lung, melanoma, bone marrow and ovary.
Interested in working with NAACCR and E-path Reporting? Please Contact Lori Havener at NAACCRlhavener@naaccr.org Or Jovanka Harrison at NYSCR jnh01@health.state.ny.us
Special Thanks To The NY State Cancer Registry (NYSCR) and DOH Colleagues for Assistance and E-path Support Amy R. Kahn, M.S., CTR Jovan Ormsby, CTR Todd Szwetkowski, CTR Maria J. Schymura, Ph.D. (Director) NYSCR Staff ECLRS Help Desk Ron Fleming Dave DiCesare Charleen Cox NYS Department of Health IT Support Staff Charles Fisher Charlie DiDonato Hans Proske Wadsworth Labs Mary Claire Aitken Debbie A. Raucci All Clinical Evaluation Program (CLEP) Surveyors
Acknowledgment This work is supported in part by the Centers for Disease Control and Prevention’s cooperative agreement U58/DP000783 awarded to the New York State Department of Health.
HL-7 - the 7th Layer of ISO’s Communications Model “Health Level-7” – highest level of the International Organization for Standardization (ISO) Open System Interconnection (O.S.I.) communications model- 1- Physical - (Bluetooth) 2- Data Link - (frame relay, ethernet) 3- Network - (internet protocol- IP) 4- Transport- (transmission control protocol-TCP) 5- Session - (network basic input/output system-NetBios) 6- Presentation - (multi-purpose internet mailextensions-MIME; SSL) 7- Application Layer-(http, ftp, Telnet) HL-7 focuses on application layer protocols for the health care domain.

![Nasopharyngeal Cancer [6]](https://cdn1.slideserve.com/3354426/nasopharyngeal-cancer-6-dt.jpg)