Download
1 / 18
180 likes | 232 Views
Delirium Amnestic syndrom. MUDr.Tomáš Kašpárek Dep. of Psychiatry Masaryk University, Brno. Delirium. Characteristics. transient cognitive disorder core features : impairment of consciousness with attention deficit, rapid onset , fluctuating course .

E N D
DeliriumAmnestic syndrom MUDr.Tomáš Kašpárek Dep. of Psychiatry Masaryk University, Brno
Characteristics • transientcognitive disorder • core features: impairment of consciousness with attention deficit, rapid onset, fluctuating course. • other phenomena may appear more prominent, but are not always present • psychomotor changes (agitation), perceptual changes as illusions and hallucinations, disorganized thought, delusions, disturbances of sleep, emotional changes (irritability, flatness of emotions)...
Historical notes • middle ages: phrenitis, frenzy, febrile insanity • 19th century: • „clouding of consciousness“ – lack of clarity of what it means • „confusion“ – lack of specificity to delirium • „amency“/acute confusuinal state – terms describing milder states of delirium, obsolete • 50s: attentional and other cognitive abnormalities are core features, associated with slowing on the EEG
Risk factors • severity of physical illness • older age • baseline cognitive impairment (dementia)
Etiology • manifestation of brain dysfunction due to systemic or brain disease or drug intoxication or withdrawal; often summation of causes • intoxication - anticholinergics, lithium, hypnotics, alcohol • withdrawal – hypnotics, alcohol • tumor • trauma, subdural hematoma • infection – cerebral, systemic • cardiovascular – cerebrovascular, cardial • metabolic – hypoxemia, electrolyte disturbances, renal or hepatic failure, hyper/hypoglycemia • endocrine – thyriod, glucocorticoid disturbances • nutritional – thiamin, B12 deficiency
Diagnosis • Delirium due to general medical condition • Substance intoxication delirium • Substance withdrawal delirium • Delirium due to multiple etiologies • CRITERIA • Disturbance of consciousness (reduced clarity of awareness of the environment) with reduced ability to focus, sustain ro shift attention • A change in cognition (memory - recent, language, disorientation) or a perceptual disturbance not due to pre-existing dementia • rapid onset and fluctuating course
Differential diagnosis • Dementia • include temporal factor (onset, course, progression) • no alteration of consciousness • Psychotic, mood, anxiety disorders • no alteration of consciousness
Treatment • Treatment of primary medical condition • minimizing doses of all sedative and psychoactive medications (except of alcohol or sedative withdrawal delirium) • symptomatic control of agitation • high potency AP (haloperidol) • avoid low potency AP and sedative agents (benzodiazepines, antihistaminics) – worsening!!! • severe, life threatening agitation – sedation with controlled ventilation
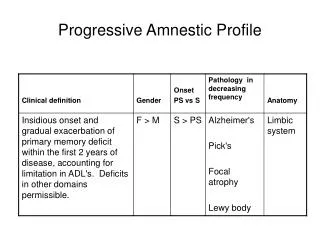
Characteristics • Definition: acquired impaired ability to learn and recall new information (and past events sometimes) • No attention deficit or clouding of consciousness (delirium), no other cognitive dysfunction (dementia) • Secondary syndromes caused by systemic medical or primary cerebral diseases, substance abuse disorders, medical adverse effects
Historical notes • Korsakoff • alcoholic psychosis, ie severe disturbance of mental status • DSM III, III-R • memory impairment (short, long-term memory) • DSM IV • key feature = impaired learning • distinction vs. dementia: dementia = multiple impairment • transient vs. chronic forms (breakpoint = 1 month)
Etiology • Diencephalic and middle temporal lobe structures (mammillary bodies, hippocampus) • Causes of amnestic syndrome: • closed head trauma • penetrating missile wounds • focal tumors • surgical intervention • herpes simplex encephalitis • infarction of the territory of the posterior cerebral artery • hypoxia • chronic use of alcohol with thiamine deficiency • Transient forms – linked with CVS disorders, pathology in the vertebrobasilar system, episodic physiologic or metabolic disorders, acute intoxications, seizures
Diagnosis • Amnestic disorder due to a General Medical Condition • Substance-induced persisting amnestic disorder • CRITERIA • development of memory impairment as manifested by impairment in the ability to learn new information or the inability to recall previously learned information • significant impairment in social or occupational functioning due to the memory impairment • memory disturbance does not occur exclusively during the course of delirium or dementia
Differential diagnosis • Delirium • memory impairment in the context of impaired consciousnes and reduced ability to sustain, focus ro shift attention • but – amnestic disorder may emerge from delirium (Korsakoff´s syndrome) • Dementia • coexistence of memory impairment with multiple cognitive deficits • Dissociative amnesia • lack of impaired learning new information – circumscribed inability to recall previously learned information with normal functioning in the present
Clinical notes • Transient global amnesia • episodes of transitory inability to learn new information (to form memories) • variable inability to recall memories from the episode • restoration to completly intact cognitive state • no behavioral changes x may be confusion, perplexity • sudden/gradual onset – according to the cause (head trauma, CNS event, chronic toxic exposure) • disorientation – may be to place and time due to severe mnestic disorder x spared orientation to person (dementia) • lack of insight • confabulations
Treatment • No effective treatments for amnestic disorder aimed specifically at learning deficit • Treat underlying pathological process • rehabilitation after brain injury
References : • Waldinger R.J.: Psychiatry for medical students, Washington, DC : American Psychiatric Press, 1997 • Kaplan HI, Sadock BJ, Grebb JA.: Kaplan and Sadock´s synopsis of psychiatry, Baltimore: Williams and Wilkins, 1997