Download
1 / 14
140 likes | 237 Views
R Dhangana , TP Murphy, MJ Pencina , MB Ristuccia , JV Cerezo , D Tsai

E N D
R Dhangana, TP Murphy, MJ Pencina, MB Ristuccia, JV Cerezo, D Tsai Prevalence of Low Ankle-Brachial Index, Elevated Plasma Fibrinogen and CRP Among Those Otherwise at Low-Intermediate Cardiovascular Events’ Risk: Data from the National Health and Nutrition Examination Survey (NHANES) 1999-2004
Disclosure Information • No Financial, Commercial, or any other conflict of interest for any author.
Introduction • Deaths and percentage of total death for the 10 leading causes of death: United States, 2002-2003. National Center of Health Statistics. • Heart Attack and Angina Statistics. American Heart Association (2003). • Myerburg RJ, Kessler KM, Castellanos A. Sudden cardiac death: epidemiology, transient risk, and intervention assessment. Ann Intern Med 1993; 119:1187-97. • CHD is highly prevalent and responsible for 1 in 5 deaths in US1. • 1.2 million people suffer coronary attack every year; about 40% die as a result of the attack2. • While primary medical prevention is shown to be very effective, at least 25% of MIs or sudden cardiac deaths occur with little prior warning of cardiovascular disease risk3. • Identifying people for prevention is important
Introduction • Risk assessment is usually done using Framingham Risk variables • 75% of adults are low-intermediate risk • But 85% of MI’s/sudden deaths occur in low-intermediate risk • Abnormal ABI, elevated plasma fibrinogen and plasma CRP levels have been shown to be associated with increased risk of CHD events and mortalityeven in those at low-intermediate CHD risk1-3. • However, prevalence estimates of abnormal ABI, fibrinogen and CRP among those not considered at high risk for CHD events have not been reported. • Fowkes FG, Murray GD,, et al. JAMA 2008; 300:197-208 • Danesh J, Lewington S, et al. JAMA 2005; 294:1799-809. • Montecucco F, Mach F. Clin Interv Aging 2008; 3:341-9.
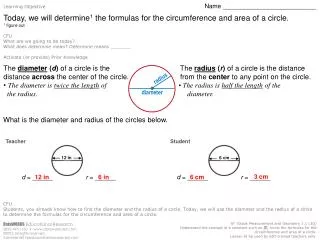
OBJECTIVES To obtain U.S. population prevalence estimates for abnormal ABI, fibrinogen, and/or CRP for individuals without known “CHD-equivalence” with low or intermediate Framingham Risk score having
Definitions • “High” Framingham Risk: >=20% 10-year risk of heart attack or coronary sudden death • Population without “CHD equivalence”: no history of coronary heart disease or stroke, and without diabetes) • Abnormal ABI=ABI <0.9 in either leg • Elevated plasma fibrinogen (>=400 mg/dl) • Elevated plasma CRP (>3mg/L)
STUDY POPULATION • Data from 1999-2004 NHANES • NHANES: a large, multicenter survey of the U.S. civilian non-institutionalized population conducted by NCHS of CDC • Population sampled to be representative of the overall U.S. population.
INCLUSION CRITERIA • Age 40 and older • ABI, fibrinogen, CRP and FRS variables available • Participants with hx of diabetes, CHD, stroke or atherosclerotic vascular disease were excluded from further analyses. • After all exclusions →→ 6,292 men and women were included.
Interviews & Physical Examinations • Histories and Physical Examinations • Blood tests and ankle brachial index • Standard ABI methods
STATISTICAL METHODS FRS was calculated based on the use of “Framingham” risk factors tables1-2 applied to NHANES data. Prevalence estimates (with CIs) were determined for abnormal ABI, fibrinogen and CRP in low-int FRS and high FRS categories. 1. NHANES: Analysis and Reporting Guideline (http://www.cdc.gov/nchs/data/nhanes/nhanes_03_04/nhanes_analytic_guidelines_dec_2005.pdf). 2. Anonymous. ATP III final report. Circulation 2002; 106:3143-421.
Prevalence of ABI < 0.9, elevated fibrinogen (>=400 mg/dl), and elevated CRP (>3mg/L) in Adults Aged 40 years and older, NHANES 1999-2004; n = 6292* *No known prevalent history of CHD, Stroke, Diabetes, or Atherosclerotic Vascular Disease Results
Framingham Risk Score vs. ABI: n = 5459 P-value <.0001 Framingham Risk Score vs. Fibrinogen: n = 6292 Results P-value <.0001 Framingham Risk Score vs. CRP: n = 6292 P-value <.0012
FRS vs. either abnl ABI or Fibrinogen or CRP : n = 6292 Results P-value <.0001
CONCLUSION Prevalence of abnl ABI, fibrinogen, CRP is high even in those without “high FRS” This is known to correlate with increased events despite “low-intermediate” risk Use in screening could be effective and improve public health