Download
1 / 1
10 likes | 57 Views
Understanding the sequence of conflict & containment events: CONSEQ. Seclusion & time out

E N D
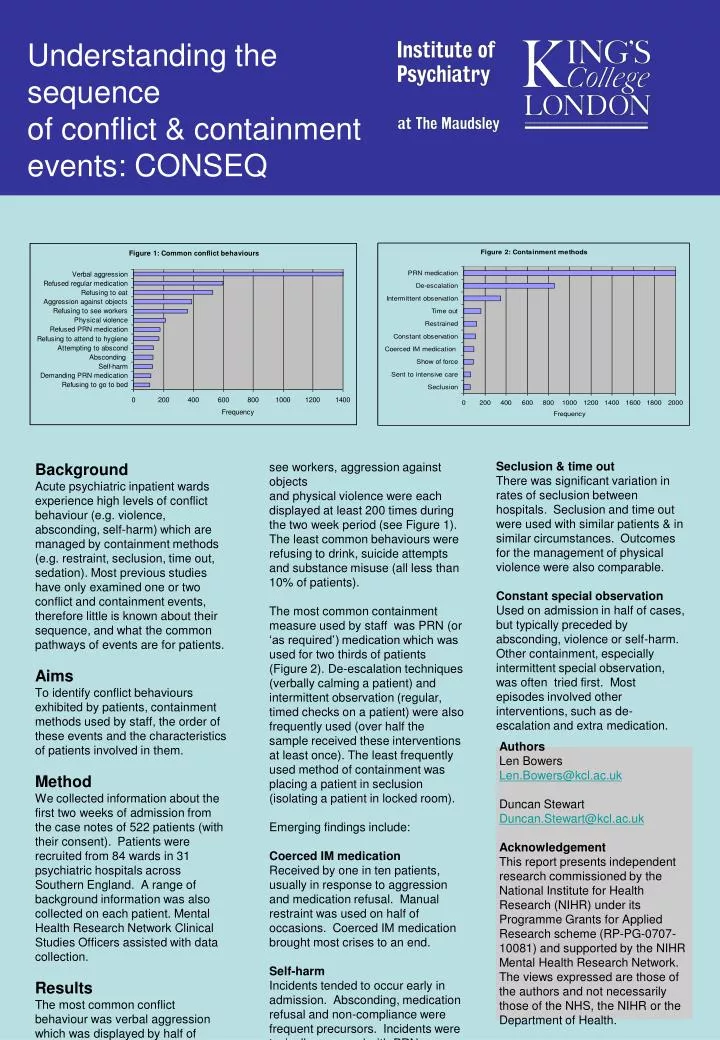
Understanding the sequenceof conflict & containment events: CONSEQ Seclusion & time out There was significant variation in rates of seclusion between hospitals. Seclusion and time out were used with similar patients & in similar circumstances. Outcomes for the management of physical violence were also comparable. Constant special observation Used on admission in half of cases, but typically preceded by absconding, violence or self-harm. Other containment, especially intermittent special observation, was often tried first. Most episodes involved other interventions, such as de-escalation and extra medication. Background Acute psychiatric inpatient wards experience high levels of conflict behaviour (e.g. violence, absconding, self-harm) which are managed by containment methods (e.g. restraint, seclusion, time out, sedation). Most previous studies have only examined one or two conflict and containment events, therefore little is known about their sequence, and what the common pathways of events are for patients. Aims To identify conflict behaviours exhibited by patients, containment methods used by staff, the order of these events and the characteristics of patients involved in them. Method We collected information about the first two weeks of admission from the case notes of 522 patients (with their consent). Patients were recruited from 84 wards in 31 psychiatric hospitals across Southern England. A range of background information was also collected on each patient. Mental Health Research Network Clinical Studies Officers assisted with data collection. Results The most common conflict behaviour was verbal aggression which was displayed by half of patients at least once during their first two weeks of admission. Refusing to eat, refusing to see workers, aggression against objects and physical violence were each displayed at least 200 times during the two week period (see Figure 1). The least common behaviours were refusing to drink, suicide attempts and substance misuse (all less than 10% of patients). The most common containment measure used by staff was PRN (or ‘as required’) medication which was used for two thirds of patients (Figure 2). De-escalation techniques (verbally calming a patient) and intermittent observation (regular, timed checks on a patient) were also frequently used (over half the sample received these interventions at least once). The least frequently used method of containment was placing a patient in seclusion (isolating a patient in locked room). Emerging findings include: Coerced IM medication Received by one in ten patients, usually in response to aggression and medication refusal. Manual restraint was used on half of occasions. Coerced IM medication brought most crises to an end. Self-harm Incidents tended to occur early in admission. Absconding, medication refusal and non-compliance were frequent precursors. Incidents were typically managed with PRN medication and de-escalation. Authors Len Bowers Len.Bowers@kcl.ac.uk Duncan Stewart Duncan.Stewart@kcl.ac.uk Acknowledgement This report presents independent research commissioned by the National Institute for Health Research (NIHR) under its Programme Grants for Applied Research scheme (RP-PG-0707-10081) and supported by the NIHR Mental Health Research Network. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.






















