Download
1 / 32
320 likes | 474 Views
Eosinophilic Respiratory Problems: Allergic Bronchopulmonary Aspergillosis. Paul A. Greenberger, M.D. 6 December 2011 Workshop 12. Objectives. To review the differential diagnosis of pulmonary eosinophilia in patients with asthma

E N D
Eosinophilic Respiratory Problems: Allergic Bronchopulmonary Aspergillosis Paul A. Greenberger, M.D. 6 December 2011 Workshop 12
Objectives • To review the differential diagnosis of pulmonary eosinophilia in patients with asthma • To discuss classification of Allergic Bronchopulmonary Aspergillosis (ABPA) • To consider treatment options for ABPA-corticosteroids, anti-fungals, and immunomodulators
Minimal Diagnostic Criteria for ABPA-Central Bronchiectasis (ABPA-CB) • Asthma • Central bronchiectasis • Immediate cutaneous reactivity to Aspergillus species or A. fumigatus • Elevated total serum IgE (>417 kU/L) • Elevated serum IgE-A.fumigatus and or IgG-A.fumigatus compared to sera from prick positive patients with asthma
Populations at Risk of ABPA • Asthma, mild intermittent to persistent severe asthma-about 1% of persistent asthma patients – diagnosed before age 20 but can be found in children and even geriatric patients. (Dx may be overlooked for decades) • Cystic Fibrosis- from 1-14% in literature; ABPA may worsen the course of CF (air trapping, airway narrowing, unequal ventilation)
The Genus Aspergillus Has Over 180 Species • There are 22 recognized recombinant Aspergillus allergens by the IUIS designated Asp f 1 to Asp f 29. Molecular weights 11-90 kD. • Four of the 22 include 2 from A. niger and 1 from A. oryzae and 1 from A. flavus. • Approximately 40 components of A.fumigatus bind to IgE antibodies.
A. fumigatus- Characteristics • Ubiquitous-outdoor recoveries even in winter • Thermotolerant • High numbers of spores occur after exposure to moldy hay, compost piles, potting soil, moldy wood chips, decaying vegetation, crawl spaces and basements, etc
Question: What fungi grow in bird droppings? • ___________________ • ___________________ • ___________________ • ___________________
In The Indoor Environment, Aspergillusfumigatus Can Be Recovered In/From • Bedrooms Yes No ? • Hallways Yes No ? • Bathrooms Yes No ? • Water supply Yes No ?
Normal Defenses Against Inhaled A. fumigatus Spores • Alveolar macrophages-ingest and kill spores • PMNs-kill by an oxidative burst • Pulmonary epithelium-as a barrier • Alternative pathway of Complement-C3 and C5 • Platelets
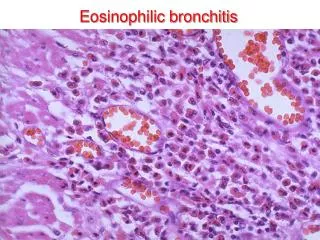
Presentation of ABPA • Asymptomatic pulmonary infiltrate • Pulmonary infiltrate(s) with eosinophilia • Worsening asthma • Peripheral blood eosinophilia • Inspisated mucus difficult to remove during bronchoscopy.. • Minimal cough or wheeze (or no asthma)
Complications of ABPA • End Stage fibro-cavitary lung disease-Pseudomonas pneumonias, chronic sputum production, home O2 • Deaths, lung transplants • Worsening of asthma from mild to prednisone dependent
Asthma with middle lobe syndrome Severe asthma with fungal sensitization (SAFS) Asthma with community acquired pneumonia Chronic eosinophilic pneumonia Churg-Strauss Syndrome Mucoid impaction syndrome ABPMycosis Bronchocentric granulomatosis Hyper IgE Syndrome Chronic Granulomatous Disease Parasitism (Ascaris, Strongyloides etc) Cystic Fibrosis Idiopathic Bronchiectasis Obejctive 1: Differential Diagnosis
Randomized Controlled Trial of Oral AntifungalTreatment for Severe Asthma with Fungal SensitizationThe Fungal Asthma Sensitization Trial (FAST) Study • AJRCCM 2009;179:11-18 • Patients with SAFS do not fulfill criteria for ABPA • Criteria for SAFS…. • 1. severe (poorly controlled) asthma, 2. total IgE concentration < 1000 IU/mL (< 1000 kU/L) 3. skin test + or elevated in vitro IgE to ANY fungus
Two Categories of ABPA • ABPA-Central Bronchiectasis (ABPA-CB) with bronchiectasis present on inner 2/3 of CT field • ABPA-Seropositive (ABPA-S)-which is a less aggressive form (Ann Allergy 1993;70:333-338) • ABPA-S can convert to ABPA-CB
Classification of ABPA • ABPA with central bronchiectasis …..ABPA-CB • ABPA without bronchiectasis………….ABPA-S • ABPA with “other radiologic findings”..ABPA-ORF • ABPA is classified into 5 stages for ABPA-CB and 4 stages for ABPA-Seropositive • Patients can change stages over time in either direction except if stage 5 (end stage- fibrocavitary)
Objective 3. Treatment Options • Oral Corticosteroids • Anti-fungals • Immunomodulators • TREAT the ASTHMA and CO-MORBIDITIES • CONSIDER ENVIRONMENTAL SOURCES
Prednisone as Monotherapy • 0.5mg/kg/each am for 2 weeks then on alterate mornings for 2 months….then • Taper prednisone • Repeat HRCT examination • Repeat total IgE (should decline at least by 33%) • Environmental exposures to molds-inquire re home and workplace for obvious sources
Antifungals • Oral (itraconazole, voriconazole, posaconazole) • Adverse effects of itraconazole…Gastrointestinal intolerance, LFTs, headache, peripheral neuropathy, sleep disturbance….and inhibition of CYP 3A4 dependent hepatic metabolism (increases concentration of prednisolone (not prednisone) and inhaled budesonide and fluticasone causing HPA suppression)
Itraconazole is a POTENT INHIBITOR of medications metabolized via CYP3A4 • Potentiation of budesonide 400 ug/day in 2 weeks leading to adrenal suppression (J Cyst Fibrosis 2003;2: 73-5) • Methylprednisolone • Statins • Cyclosporine
Anti-inflammatory effect of itraconazole in stable allergic bronchopulmonary aspergillosis: A randomized controlled trialJACI 2003;111:952-7 • Itraconazole 400 mg daily for 16 weeks • Primary outcome was induced sputum eos • Secondary outcome measures: TEC, total IgE concentration, IgE-A fumigatus by CAP • No pt had a change in LFTs • Baseline FEV1 % = 55 (itraconazole) and 52 (placebo)
Outcomes • Induced sputum eos: 3.8% decreased to 0.4% vs 3.0 to about 2% in controls • Sputum ECP 4900 ng/ml decreased to 3000 in 4 weeks vs 3400 increased to 3600 in controls • Thus, sputum eos are reduced with itraconazole; sputum ECP follows suit
Clinical Markers • Asthma exacerbations: 0 if itraconazole vs 1.5 for controls over 16 weeks • No improvement in FEV1 • Conclusions: There are reductions in AIRWAY INFLAMMATION (induced sputum eos and sputum ECP) with itraconazole
Voriconazole • Improved oral bioavailability than itraconazole • Peripheral blood concentrations have……….100 fold interpatient variability vs 15 fold with itraconazole! • Adverse effects of hepatic, ophthalmologic, photosensitivity • Dosage in adults <65 yrs is 200mg bid
VORICONAZOLE THERAPY IN CHILDREN WITH CYSTIC FIBROSIS J Cyst Fibrosis 2005;4:215-20 • 21 CF children (ages 5-16 yrs) • Monotherapy in 2 children, sustained improvement for 13 months • Combined with steroids in 11 children with improvement • Monotherapy in Af colonized, non-ABPA pts-no change in symptoms • Adverse effects: 7 (33%) including photosensitivity, nausea, LFTs, alopecia
Question: The T ½ of Serum IgE is • 6 days • 5 days • 23 days • 2.3 days • 14-21 days
Omalizumab • Case reports (some +, some -) • Controlled trial for CF-ABPA initiated
Steroid dependency despite omalizumab treatment of ABPA in cystic fibrosis AllergyVolume 65, Issue 1, pages 134-135, 5 OCT 2009 DOI: 10.1111/j.1398-9995.2009.02147.xhttp://onlinelibrary.wiley.com/doi/10.1111/j.1398-9995.2009.02147.x/full#f1