Download
1 / 34
340 likes | 467 Views
Antioxidant therapy in hemodialysis patients: a systematic review. Kidney International (2012) 81, 233–246 報告者: Fellow 1 陳筱惠 指導 醫師 :尤俊成醫師. BACKGROUND. Oxidative stress: Pro-oxidants overwhelm antioxidant defenses. Pro-oxidants: reactive oxygen species and reactive nitrogen species

E N D
Antioxidant therapy in hemodialysis patients: a systematic review Kidney International (2012) 81, 233–246 報告者:Fellow 1 陳筱惠 指導醫師:尤俊成醫師
BACKGROUND • Oxidative stress: • Pro-oxidants overwhelm antioxidant defenses. • Pro-oxidants: reactive oxygen species and reactive nitrogen species • Consist of free radicals • Most common reactive nitrogen: nitric oxide • Antioxidants: synergistic relationships • Endogenous • Exogenous • Dietary: vitamin E (a-tocopherol), vitamin C (ascorbic acid), and b-carotene • Therapeutic: N-acetylcysteine and bardoxolone
The markers of oxidative stress: • F2-isoprostanes,lipid hydroperoxides, oxidized anti-LDL antibodies, the oxidizability of LDL, free sulfhydryl groups, carbonyl groups, 3-chlorotyrosine, and advanced oxidation protein products
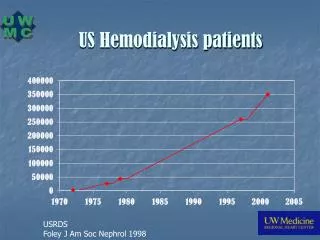
Oxidative stress in HD patients: • HD patients have elevated oxidative stress compared with healthy matched controls. • Contribute to the high levels of CVD morbidity and mortality in these individuals • Plasma levels of vitamin E are decreased during HD.
decreasing uptake of dietary antioxidants HD activate immune cells and increases production of reactive oxygen species
Cardiovascular disease (CVD): • 10~20 fold increased risk, cause of death in ~34% of hemodialysis (HD) patients • Interventions aimed at improving CVD outcomes in HD patients: • Lipid-lowering therapy • Increased dialysis dose • About the timing of dialysis initiation • Antioxidant therapy positive effect
Antioxidants and cardiovascular disease • Beneficial effects in following studies: • Observational studies: • World Health Organization’s MONICA (MONitoring trends and determinants In CArdiovascular disease) Study • The Nurses Health Study • The US Physicians study • Randomized controlled clinical trials: CHAOS (Cambridge Heart AntiOxidant Study) • Large trials ?? • HOPE (Heart Outcomes Prevention Evaluation) trial1 • The Heart Protection Study
SYSTEMATIC REVIEW -- Methods • PubMed • Search terms: dialysis and • Aantioxidants, vitamin E, tocopherol, vitamin C, ascorbic acid, selenium, acetylcysteine, vitamin A, beta-carotene, coenzyme Q10 • Limits: humans and clinical trials that investigate effects of oral antioxidant therapy on a marker/s of oxidative stress or a CVD outcome measure in patients undergoing HD • 56/298 articles: • 53 studies the effects of antioxidant therapy on a biomarker or biomarkers of oxidative stress • 3 studies the effects of antioxidants on CVD end points
SYSTEMATIC REVIEW -- General considerations • The timing of blood collection for oxidative stress biochemical measures • 35/53studies Comparing predialysisdata: blood samples shortly after initiation of the HD session, before and after the therapeutic period • 9/53 studies Comparing changes from pre- to postdialysis: change in the measures before and after the dialysis session, before and after the therapeutic period • 4/9 studies Comparing postdialysis: changes in oxidative stress from postdialysis, before and after therapy
Substrates with oxidative damage: 20 oxidative stress biomarkers • Lipids (44 studies): • 1st: Malondialdehyde(MDA), 27 studies • 2nd: LDL cholesterol, 10 studies • 3rd: isoprostanes, 4 studies; protein carbonyls, 4studies) • 4th: lipid hydroperoxides, 3 studies • Proteins (7 studies) and DNA (1 study)
FINDINGS • 37/53 studies: a decrease in biomarkers of oxidative stress following antioxidant therapy (20/37 a-tocopherol) • 15/53 studies: no effect • 8/53 studies: anincrease
a-Tocopherol • 25 studies investigating the effects of a-tocopherolon oxidative stress in HD patient • 20/25 studies: decrease oxidative stress • The mean dose: 500 mg/day (15~1200 IU/day) • 5/25 studies showing that a-tocopherolhad no effect: • The doses: 200 mg/day, 800 IU/day
The form of a-tocopherol: natural or synthetic?? • The majority of studies did not specify the form administered. • Duration: • No differences in the median duration of therapeutic periods in the studies showing that a-tocopheroldecreased oxidative stress compared with those reporting no effect • 8 weeks
3/25 studies: RCT design, 95 patients • Effects of atorvastatin and vitamin E on lipoproteins and oxidative stress in dialysis patients: a randomised-controlled trial. J Intern Med 2005; 257: 438–445 • a-tocopherol (800 IU/day) + atorvastatin (40 mg/day), 12 weeks • No effect of a-tocopherolon plasma-oxidized LDL
Effect of vitamin E therapy on oxidative stress and erythrocyte osmotic fragility in patients on peritoneal dialysis and hemodialysis. J Nephrol 2006; 19: 739–745 • 800 IU/day, 6 months • No effect on oxidative protein products • Serum vitamin E and oxidative protein modification in hemodialysis: a randomized clinical trial. Am J Kidney Dis 2007; 50: 305–313 • 300 mg/day, 20 weeks • Decreased erythrocyte osmotic fragility and plasma MDA
Vitamin C • 11studies, 371 patients, 9 with RCT design • 4/11 studies: decrease oxidative stress • 250 mg 12 weeks, 1g/day 1 year, orally • 300 mg~1 g/day 8 weeks, intravenously • 3/11 studies: increase oxidative stress • 2/3 studies: a single intravenous dose • Vitamin C with metal ions that may exacerbateoxidative stress (may occur after single dose). Over time, there are adjustments to defenses that eventually result in a more pronounced antioxidant effect.
1/3 studies: 200mg~1 g/day, 3 months • The increased dose may have a similar effect as the single dose, with insufficient time to enable other antioxidant defenses to compensate. • 4/11 studies: no significant effect • 250mg/day, 4~12 weeks, ineffectual period and dose
N-acetylcysteine • Increase the endogenous antioxidant glutathione by contributing cysteine • Facilitate the production and action of nitric oxide, leading to improved vasodilation • 4 studies. 172 patients, 3 with RCT design • All studies: decrease oxidative stress • 1.2, 2, 5 g/day • One-off dose, 3 weeks
Selenium • Essential trace element that functions as a cofactor for the reduction of antioxidant enzymes such as glutathione peroxidase, but toxic in large doses • 3 studies, 40 patients • 2/3 studies: decrease biomarkers of oxidative stress • 1/3: no effect • 25ug orally, 400mg intravenously, 8~20 weeks
Other antioxidants • r-tocopherol • Docosahexaenoic acid • a-lipoicacid • Coenzyme Q10
Antioxidant combinations • 7 studies, 1 with RCT design • 4/7 studies: decrease oxidative stress • 2/7 studies: no effect • 1/7 studies: a decrease in one biomarker, but no change in another • 6/7 studies with a-tocopherol, 5/6 studies with vitamin C
Clinical outcome trials • 3 trials • The effect of vitamin C supplementation and withdrawal on the mortality and morbidity of regular hemodialysis patients. ClinNephrol1989; 31: 31–34 • The 1st clinical outcome trial in HD patients • Noncontrolled, 61 patients • 500 mg/day of vitamin C, 2 years • No difference in morbidity or mortality rates
SPACE (Secondary Prevention with Antioxidants of Cardiovascular disease in End-stage renal disease) trial • This most cited one • Randomized, double-blind, placebo-controlled trial • 97 patients, 800 IU a-tocopherol/day, 500 days • 99 patients, placebo • 54% reduction in cardiovascular risk (P=0.014), 40% reduction in composite CVD end points, 70% reduction in total myocardial infarction (P=0.014 and 0.016, respectively) • Lack of a healthy control group??
The antioxidant acetylcysteine reduces cardiovascular events in patients with end-stage renal failure: a controlled trial. Circulation 2003; 107: 992–995 • 64 patients, 1.2 g/day orally, 14months • 70 patients with placebo • Reduced rates of CVD events, but no differences in secondary end points (total mortality and CVD mortality)
Thepresence of oxidative stress was not an inclusion criterion for 3 trials. • Patients were potentially not in a biochemical state that would benefit from additional antioxidant defenses.
FUTURE STUDIES • Lack of a clinically accepted and validated oxidative stress biomarker