Download
1 / 55
560 likes | 743 Views
PRESSURE SORES. By Dr Zahid Iqbal Bhatti Trainee Registrar. Definition. Soft tissue injuries resulting from unrelieved pressure over bony prominences. The Term “Bed sores or decubitus ulcer” should be avoided as they point out that all the sores are the result of supine position.

E N D
PRESSURE SORES By Dr Zahid Iqbal Bhatti Trainee Registrar
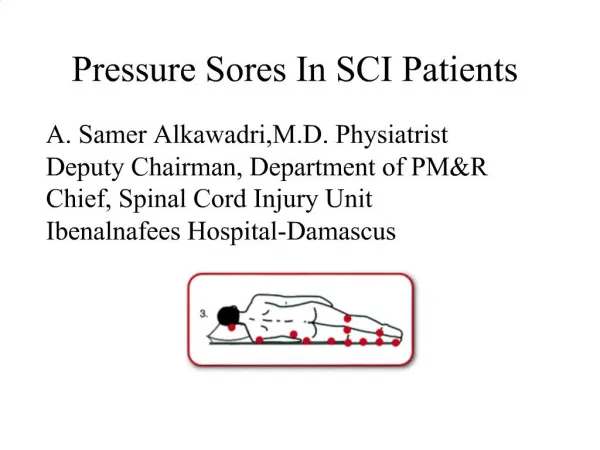
Definition • Soft tissue injuries resulting from unrelieved pressure over bony prominences. • The Term “Bed sores or decubitus ulcer” should be avoided as they point out that all the sores are the result of supine position. • In the lying position,the tissue destruction can occur over sacrum, scalp, shoulders, calves,and heels.
In the sitting or wheel chair position, the sores develop at the ischial area. • Relieving the pressure is the key factor to healing and key to prevention. • Poor nutrition, incontinence with persistent soilage and moisture, dementia, paralysis and friction make the healing less likely.
Risk factors • Age • Impaired sensory perception • Moisture • Immobility • Poor Nutrition • Friction
Stages of Pressure Sores • Stage 1. skin Intact but reddened for more than one hour after relief of pressure
Stage 2 • Blister or other break in the dermis with or without infection.
Stage 3 • subcutaneous destruction in to the muscle with or without infection • .
Stage 4 • Involvement of the bone or joint with or without infection
What is seen on the surface is often the tip of ICE BURG • In general, approximately 9% of all hospitalized develop pressure sores
Pathophysiology • Factors involved • Pressure • Infection • Edema • Altered Neurological state
Pathophysiology • Compression of the soft tissue results in ischemia and if not relieved, will progress to necrosis and ulceration even in the vascularized area • In Susceptible patients, it is accelerated by infection, inflammation and edema.
Cont- • If the external pressure exceeds capillary bed pressure, capillary perfusion is impaired and ischemia results. • There is an inverse relationship between the amount of pressure and the length of time required to cause ulceration. • .
Cont- • The initial pathological changes occur in the muscles overlying the bones followed by more superficial tissue and skin in last • Denervated and compressed skin becomes edematous which plays an important role in the pressure sore formation.
PREOPERATIVE CARE • Preparing the patient & family for long term management requires team approach: • Internal medicine • Endocrinology • Neurology • Urology • Nutritionist • Physical & occupational therapy • Psychiatry • Specialist Nurse
Cont- • Care of the pressure sore is not only the care of the wound. • It includes the systemic strategy including nutritional assessment and maintenance, control of infection both local and systemic and pressure and spasm relief.
Preoperative care • Nutrition • Treatment of infection • Relief of pressure • Management of spasm • Contracture therapy
1-Nutrition • Normal healing potential exists when the serum albumin is above 2.0 g/dl • Daily requirement of person 1.5-3.0 g/dl of protein and 25-35 cal/kg of non protein • Exercise should be added to increase protein synthesis and anabolic drive. • Vitamin C and A and Zinc .
2-Infection • Pressure sores may or may not be present with local infection • If infection present ,should be debrided either at bed site or O.R. and small amount sent for microbiology • Swabbing should be avoided • Antibiotics (Local or systemic) if infection or Escher present.
These are at the risk of UTI and RTI infections. • If present UTI treated by antibiotic and change of catheter if present. • If Pneumonia then Positioning, side to side rolling, deep breathing and chest physiotherapy with bronchodilators.
3-Relief of Pressure • This should be the prime goal. • Healing will not occur in the presence of ischemia or infection. • Frequent turning and intermittent elevation of the hips in the wheel chair • Various mattress and wheelchair padding.
Management of spasm • Most common in spinal cord injuries • 100% in cervical • 75% in thoracic • 50% in thoracolumber • Medications • Diazepam ( valium ) 10mg every 4 to 6 hours • Baclofen ( Lioresal ) 5mg every 6 hours • Dantrolene ( Dantrium ) 25mg every 12 hours.
Contracture therapy • Tightening of muscle & joint capsule • Physiotherapy • Tenotomies
SURGICAL & NON SURGICAL TREATMENT
Non surgical treatment • Some patients may never be candidate for surgical correction • due to medical problems • Avoidance of unrelieved pressure • Control of infection • Control of incontinence • Improved nutrition
Surgical treatment • Three principles • Excisional debridment of the ulcer, its bursa, and any calcification. • Partial or complete ostectomy to reduce the bony prominence. • Wound closure with healthy tissue.
1-DEBRIDEMENT • DEBRIDEMENT of any dead, necrotic tissue after instillation of methylene blue and Hdrogen peroxide . • Viable tissue specimen sent for quantitative culture • Post operatively, wound packed and dressing changed every 6-8 hrs.
2-OSTECTOMY • Removal of bony prominences in an integral part of surgical treatment of bed sores. • Radical Ostectomy avoided. • Removing minimum amount of bone necessary.
3-PRESSURE SORE CLOSURE • Considering not only the present surgery but also need for subsequent Procedure. • Choice depends upon site, size, depth and previous surgery. • Primary closure avoided. • Skin Grafting has 30% success rate. • Use of flaps
Pressure sore closure • Advantage of Musculocutaneous flap: • Excellent blood supply • Provision of bulky padding • Ability to readvance or rotate flaps to treat recurrence.
Pressure sore closure • Disadvantages: • Tissue most sensitive to external pressure. • May be atrophic in elder patients. • Functional deformity in ambulatory patients.
ISCHIAL DEFECT • Seated position • High recurrence rate 75% about. • Medially Based thigh flap • Gluteus maximus Myocutanuous flap • V-Y pattern Biceps femoris, semimembrenosis, semitendinosis • TFL flap.
SACRAL DEFECT. • Supine position • Gluteus Maximus Muscle flap. Either rotated, advanced or turn over • Transverse and vertical lumbosacral flap.
TROCHANTRIC DEFECT • Patients in lateral position esp. in hip flexion contracture. • Commonly used is TFL flap. Rotation results in T shaped junction between flap and closed donor site which is prone to dehiscence.