Download
1 / 74
800 likes | 889 Views
Evaluation and Management of Chronic Diarrhea. Joe Harkins, PA-C Gastroenterology Center of Maine EMMC Bangor, ME. OBJECTIVES. Understand definition of Chronic Diarrhea and recognize difference between osmotic and secretory types. Identify various causes of Chronic diarrhea.

E N D
Evaluation and Management of Chronic Diarrhea Joe Harkins, PA-C Gastroenterology Center of Maine EMMC Bangor, ME
OBJECTIVES • Understand definition of Chronic Diarrhea and recognize difference between osmotic and secretory types. • Identify various causes of Chronic diarrhea. • Evaluate cases of Chronic Diarrhea including history, exam, and testing. • Understand endoscopy guidelines including EGD, Colonoscopy, and Capsule endoscopy. • Determine appropriate work-up on basis of whether feces is watery, fatty, or bloody. • Choose effective treatments for respective cases of chronic diarrhea.
1st - RULE OUT CONSTIPATION • Sometimes patient thinks it is diarrhea when actually it is overflow from constipation. • Pelvic Floor Dysfunction can happen if trouble with IAS, HX abdominal/pelvic surgery, Connective tissue disorder, DM, adverse drug effects, dehydration. • Check upright KUB for fecal loading.
RED FLAGS • Fever • Blood Loss • Unexplained weight loss • Abdominal Pain • Nocturnal episodes • REFER TO ER OR call GI.
DEFINITION of diarrhea • Loose stools • More than 3 BM per day • Stool output weight>200 gram/day
Definition • CHRONIC diarrhea: duration > 4 weeks. • Functional Diarrhea , ROME III criteria: daytime painless diarrhea > 3months.
Pathophysiology of Diarrhea Normal: fluid input to S.I. 10 L/day absorption out of S.I. 9 L /day absorption out of Colon 0.9L /day Normal Stool: 100ml per day Input comes from: food, drinks, salivary, gastric, pancreatic, biliary, small intestine, colon. Water flows through ion transporter channels, iecAMP
Digestive Input Signals • G-cell: gastrin signals release of HCl into stomach • Enteroendocrine cells: CCK stimulates Gallbladder, pancreas, and S.I. motility. • Duodenal S-cells: Secretin stimulates release of Bicarbonate from pancreas with H20 into duodenum. • D-cell: VIP stimulates motility and pancreas. • Vagal Nerve: cholinergic GI stimulation. • T4: stimulates GI motility.
Types of Diarrhea • Osmotic • Secretory • In Practice: Watery Fatty Bloody
Osmotic Diarrhea • Unmeasured osmotic substances hold water in lumen of colon. • Improves with FASTING or elimination. • Fecal Osmolar Gradient will be >125. • If lactose intolerant, low stool pH. • Can be watery or fatty stool. • KEY here is history of lactose intolerance or laxatives.
Osmotic Diarrhea • Laxatives like PEG, Lactulose, or Magnesium salts • Fructose in our diet • Lactose ( if lactase deficient) • Sorbitol, Mannitol ( sugar free gums, drinks)
FOGFECAL OSMOLAR GRADIENT FOG= 290 – 2 {fecal Na + K} mmol/l • If <50 secretory • If > 125 osmotic • If between 50-125 overlap osmotic/secretory
Secretory Diarrhea • Amount of fluid input exceeds absorption • Not affected by fasting and can continue at night • Related to excess secretion or inadequate absorption • Related to abnormal GI motility • Stool Na and Cl will be high and FOG<50 • Can be Fatty, Watery, Bloody, Mixed
Causes of Secretory Diarrhea • Infection • Alteration of intestinal surface area • Inflammation • Dysregulation/dysmotility • Neuroendocrine tumor (NET) Note - Infections, IBD, and NET not covered in depth here
Infection • C .Diff produces enterotoxins which kill enterocytes • Cholera type infections induces cGMP ion-transporters to increase Chloride secretion • Parasites- always consider this one • Viral CMV, HIV, and HSV affect colon if immunocompromised
Altered Surface Area • Ileal resection: reduces bile salt absorption • Ileocecal resection: altered bacterial concentrations reach small bowel • Surgical scar/strictures: cause stasis • Celiac disease:reduces SI surface absorption • Inflammation: increased cytokines leads to increased wall-thickening with leakage and decreased absorption
Dysregulation • diabetic autonomic dysfunction • post-vagotomy • sympathectomy • scleroderma, associated SI diverticulosis • hyperthyroidism
Secretory Causes Watery IBS Neuroendocrine Infection IBD SIBO Microscopic Celiac DM Non-osmotic laxative Short Gut Villous adenoma Alcohol (sugar) Fatty Chronic pancreatitis EPI Celiac SIBO Cirrhosis Cholestasis Bile Salt Depletion Bloody IBD Infection Radiation Ischemia Cancer
Steatorrhea Decreased fat solubilization: inadequate bile salts micelles • Intestinal stasis: SIBO and lower duodenal pH • CP/ ZES: pancrease enzyme insufficiency or enzyme deactivation by HCL • Cholestasis decreases bile salt secretion • Cholecystectomy: increases BS secretion • Ileal resection leads to BS depletion or malabsorption
Length of Ileal resectiondetermines if fatty or watery • <100cm resected : compensated with reduced BS returned to Liver. Unabsorbed BS pull water through colon wall into lumen get watery diarrhea. OK to use cholestyramine. • >100cm resected: decompensated with no BS return to liver leading to reduced BS secretion; decreased micelle formation. May not be OK to use cholestyramine. Will get mixed fatty/watery diarrhea. Tx with low fat diet.
Inflammation • Wall-thickening • Leaky wall • Impaired absorptive transporters
Evaluation of Diarrhea • History • Medication • Physical Exam • Labs/tests • Imaging • Endoscopy
History • Stool: Duration, Frequency,Intermittent vs. continuous, affected by fasting, blood, greasy, watery, mucus, Nocturnal, incontinence. • Physical Symptoms reveal Clues and Severity • Weight loss
History • Hx Surgery, radiation therapy. • PMHx: Chronic pancreatitis, Peptic Ulcers, Thyroid disease, Diabetes, HIV. • Check Diet: caffeine, FODMAPs, lactose, alcohol, diet sweeteners. • Travel History. • Well water ( giardia). • Sick contacts.
Medications • OTC and Prescription • Vitamin C (it is an acid) • Cholinergics • Laxatives: osmotic and non-osmotic
Physical Exam • Important for severity of problem • Sometimes can give clue to etiology • flushing= carcinoid, VIPoma • cirrhosis, telangectasia= alcohol • thyroid nodules= medullary carcinoma • dermatitis= celiac disease • aphthous ulcers= inflammation • rectal exam : DRE
LABS Stool tests: • C. Diff, O&P, Cx/S • Calprotectin, Lactoferrin, FOBT, fecal WBCs • FOG( Na&K), pH, Mg ( if suspecting laxative). • Elastase • Sudan III fat stain Serology: • CBC, BMP , TSH, albumin, vitamins(A,D,E,K), INR • TTG and IgA, HLA DQ2/ DQ8 (for Celiac) • CRP, ESR • B12 and Folate ( for SIBO)
Imaging • CT with IV Contrast: colitis, enteritis, diverticulitis, pancreatic tumor. • MRE or CTE with and without contrast : small bowel inflammation, fistula. • MRCP: biliary dilatation. XR or non-contrast CT: fecal loading pancreatic calcification
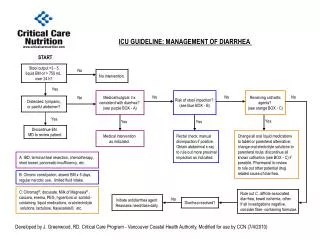
Indications for ENDOSCOPY • Colonoscopy • EGD • EUS • SI Capsule ASGE Guidelines: GIE Vol. 71, No. 6:2010
Colonoscopy • If mucus, blood, copious watery • If suspect: IBD, microscopic, serrated villous adenoma, cancer, NSAID ileitis/colitis, eosinophilic colitis. • Flexible Sigmoidoscopy : suspect distal viral or ischemia when full colon is high-risk ASGE Guidelines: GIE Vol. 71, No. 6:2010
EGD/EUS • Giardia • Gastric ulcers • ZES • Celiac • SI Crohns • Lymphangectasia • Lymphoma ASGE Guidelines: GIE Vol. 71, No. 6:2010
Small Bowel Capsule • If colonoscopy and EGD normal and suspect small bowel source for inflammation • CT and MRI may not show mucosal lesion or bleeding ASGE Guidelines: GIE Vol. 71, No. 6:2010
CASE #1: MICROSCOPIC COLITIS • 11/2015: 30 yo female presents with chronic alcohol abuse, severe neuropathy, large ascites. • She reports history of Crohns diagnosed at 26yo. Had diarrhea and colonoscopy in 2012. Tried Lialda but stopped medication. Now reports 2 BM per day. • Treated for cirrhosis and discharged to Acute Rehab for severeneuropathy.
CASE #1. MICROSCOPIC • 5/2016: f/up to GI clinic after lifeflight for UGIB with HEMATEMESIS. EGD showed Grade 1 varices. Still reports BM 2 per day. NO Crohns medication. Focus on cirrhosis. • Strength and spirit improving • Request made for Colon OP Report and PATH from 2012. Although she has HX CROHN’s, she makes no relevant complaint yet.
CASE #1. MICROSCOPIC • 9/2016: Cirrhosis now compensated, neuropathy improving. SOBER and outlook positive. NOW: She reports that for past 5 years she had 6-10 watery BM/day . No blood, no tenesmus. • Colon report 2012: lymphocytic colitis. • Look at Medication list.
CASE #1. MED LIST • Lyrica • baclofen, • ativan • MVI • Sertraline • Mag Oxide • Sertraline • melatonin • thiamine • Lasix • Synthroid • Iron • Vitamin C
Microscopic Colitis • 12/100,000 people prevalence similar to IBD • Associated: NSAIDs and PPI • Labs not necessary but fecal WBC and calprotectin are elevated ( 50-75%) • Collagenous • Lymphocytic • Secretory, Inflammatory Sleisenger & Fordtran
Lymphocytic Sleisenger & Fordtran
Collagenous Sleisenger & Fordtran
Reproduced from Munch A, Aust D, Bohr J, Et al. Microscopic Colitis: current status, present and past. Jcrohns Colitis 2012;6:932
Treatment of Microscopic Colitis • Modify Med List. {She changed to Lexapro} • Budesonide 9mgQD x 4wks, taper 3mg every weeks • Alternative: Bismuth subsalicylate 8 tabs/day x 8 weeks • Alternative: Prednisolone
CASE #1. 3RD f/up Microscopic Colitis • 12/2017 • Repeat Colonoscopy in December 2017: NORMAL • NEW Med list: • Lyrica • MVI • Mag Ox • Nadolol • Synthroid • Vistaril Doing well January 2017.
CASE #1. Microscopic Colitis Microscopic Colitis can recur. OK to retreat empirically without scope but 1st check Stool tests for infection, and blood for ESR/CRP.
CASE# 2: SIBO • 19 yo female from NH going to college in ME, active as rock climber and backcountry pursuits presents with HX diarrhea past 2 years. 4-6 per day but some days>10 per day. • Brown, watery or mushy, not greasy, No blood. Weight stable. • Frequent bloating, nausea, and occasional bilious vomit. • MED: lexapro • FM HX: Mom has IBS-C.