Download

1 / 50
530 likes | 885 Views
Dr.René TARDIVEL Etablissement Français du Sang. PLATELET TRANSFUSION IN ONCOHAEMATOLOGY. 9 th Maghreb Haematology Conference Sousse 25-26 May 2012. Indications for platelet transfusion. Central thrombocytopenia together with treatment of the cause Thrombopathy, occasional

E N D
Dr.René TARDIVEL Etablissement Français du Sang PLATELET TRANSFUSION IN ONCOHAEMATOLOGY 9th Maghreb Haematology Conference Sousse 25-26 May 2012
Indications for platelet transfusion • Central thrombocytopenia together with treatment of the cause • Thrombopathy, occasional • Peripheral thrombocytopenia, exceptional
Platelet concentrates (1) Principal characteristics
Platelet concentrates (2) Principal characteristics
Platelet concentrates (3) Storage • 5 days (7 days in certain countries in the event of bacterial detection or attenuation of pathogens) • Continuous agitation • 20-24 °C • concentration: 1.2-1.5.106/mm3 (recommendations)
Platelet concentrates (4) Possible transformations
Platelet concentrates (5) Possible qualifications
Platelet concentrates (6) CPA or MCP • No difference in effectiveness • No difference in frequency of immunization • No product superior to another, but one may be better adapted to the patient
Platelet transfusion indication Preventive or curative?
Platelet transfusion indication (1) Curative • Patient presenting a haemorrhage
Platelet transfusion indication (2) Preventive • To prevent bleeding associated with thrombocytopenia and/or thrombopathy in a curable patient or a patient with a prolonged life expectancy (bone-marrow transplant, induction of L A,…)
Platelet transfusion - PreventiveDose (1) Numerous studies seems to show the advantage of strong doses of 4 to 5 10 11 • Norol F and coll: Platelet transfusion has dose response study Blood 1998; 98:1448 - 1453 • Klumpp TR and coll: Clinical consequences of alterations in platelet transfusion dose: prospective, randomized, double-blind trial transfusion 1999; 39:674 - 681 • Sensebe et al: The efficacy of high-dose patient transfusions of platelets in hematology thrombocytopenic patients: result of prospective, randomized, open blinded end point (PROBE) study Blood 2005 105: 862-864
Platelet transfusion - PreventiveDose (2) However, other studies show that a low dose 2-3 1011 can also be effective • Tinmouth A et al: Low-dose prophylactic platelet transfusions in recipients of an autologous peripheral blood progenitor cell transplant and patients with acute leukemia: a randomized controlled trial with sequential Bayesian design. Transfusion 2004; 44: 1711-1719. • Heddle NR et al (Best ISBT Working party) Study STOP low dose 1.5 -3.1011 versus standard amounts 4-6.1011. Study stopped in 2008 because of the higher frequency of haemorraging in the low-dose group • Slichter S et al: Dose of Prophylactic Platelet Transfusions and Prevention of Hemorrhage N England journal of medicine 2010; 362:600 - 613
Platelet transfusion - PreventiveDose (3) Study PLADO (Optimal Platelet Dose Strategy for Management of Thrombocytopenia) • 3 doses of platelets: 1.1-1011/m2 2.2-1011/m2 4.4-1011/m2 • Low doses involve a reduction in the transfused platelets but increases the number of transfusions (5 versus 3 for average and high doses) • Weak or strong doses do not have an effect on the frequency of the bleedings • No significant difference when with the number of days before appearance of grade 2 bleeding or higher, no matter what the dose
Platelet transfusion - Preventivetransfusional thresholds (1) Pietersz R.N.I International Forum –Prophylactic platelet transfusion – Vox Sanguins 2012 14 responses by different countries • In the absence of risk factor 10.109/l (except Russia and in certain indications from Japan and the Netherlands: 5-109/l
Platelet transfusion - Preventivetransfusional thresholds (2) • In the event of risk factors Fever >38.5°C, evolutionary sepsis, coagulation anomaly, thrombopathy, anaemia, mucite, extensive purpura, haemorrhage inside the eye, HTA, anatomical lesions Threshold up to 20.109/l
Platelet transfusion - Preventivetransfusional thresholds (3) • Other situations Invasive techniques: catheter, implantable chamber, fibroscopy, biopsy, broncho-alveolar washing Surgery, severe haemorrhage, CIVD,… Threshold raised to 50.109/l or above
Platelet transfusion Dose in practice • Recommendation AFSSaPS or ANSM • 0.5.1011 for every 7 kg of patient weight • (or average dose suggested in PLADO study)
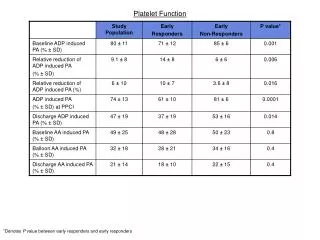
Platelet transfusion Evaluation of effectiveness - Curative: Stopping bleeding - Preventive: Increase in platelet count after transfusion Duration of transfusional effectiveness (3-4 days) Prevention of thrombocytopenia-related haemorrhages RTP > 20% and/or CCI > 7
Platelet transfusion yield (PTY) • [PC after transfusion-PC before transfusion] X weight (kg) X 0.075 • PTY = • Number of platelets transfused (X 1011) • PC: platelet count
Corrected Count Increment (CCI) • [PC after transfusion - PC before transfusion] X body surface area (m2) X 100 • CCI= • Number of platelets transfused (X 1011) PC: platelet count
Data EFS Bretagne CHU Rennes Oncohaematology (Pr. Thierry Lamy) Follow-up of the output of platelet transfusion
Study of transfusion efficiency after transfusions of single donor-apheresis platelet concentrates and random-donor platelet concentrates J.VASSE, R.TARDIVEL, S.GAUCHERON, G.ANDREU, G.SEMANA June 2007
RESULTS (1) • From 05/05/2005 to 09/04/2007 • 3496 platelet transfusions • 2354 SD-APC • 1141 RD-PC
Distribution of the plates transfused according to age (N = 11207) (08/02/2010-13/05/2012) J1 J2 J3 J4 J5 3.3% 20.5% 28% 34% 14.2% Distribution CPA/MCP CPA: 41% MCP: 59%
Tests de Comparaison des moyennes : utilisation du t de Student. La valeur de ce test doit être supérieure à 1.96 pour accepter à 95% l’hypothèse selon laquelle les moyennes observées sont différentes. • Statistiquement, nous pouvons appliquer ce test de Student après avoir vérifié l’homogénéité des variances. Le test de Fischer-Snedecor nous permet de valider cette homogénéité car dans chacun des cas, le rapport de la variance la plus élevée sur la variance la plus faible est inférieur à la valeur théorique de 1.57. • Comparaisons des moyennes : • CPA Intersol et CPA Plasma : F=1.15 et t=5.5 les moyennes sont différentes. • CPA SSP+ et CPA Plasma : F=1.18 et t=1.2 les moyennes sont identiques. • CPA SSP+ et MCP SSP+ : F=1.22 et t=0.5 les moyennes sont identiques. • MCP SSP+ et CPA Plasma : F=1.03 et t=1.1 les moyennes sont identiques.
En jaune, les moyennes significativement différentes : • J5 rendement moindre que J4 pour CPA Plasma • CPA/MCP SSP+ : les moyennes de rendement à 1 jour près peuvent sembler décroître selon l’ancienneté du PSL, mais statistiquement ces moyennes comparées au jour près sont identiques et ne présentent pas de différence. La valeur du t de Student ici compare le rendement moyen de l’âge du PSL sur la ligne concernée avec la ligne juste au dessus : ex : J5 vs J4
Results • 4459 PC Transfusions • 1219 Recipients • 2264 yeld > 20% ( 60% PC Transfusions)
Platelet transfusion Inefficiency if output < 20% or CCI <7 • Platelet concentrate • Insufficient dose • Altered platelets (transport, conservation… c.f. index of spinning) • Plaquettes proches date de péremption • Incompatible ABO • Patient • Fever, CIVD, splenomegaly, drug • Alloimmunisation HLA or HPA = refractory state (polytransfused, multipair)
Platelet transfusion Refractory state Output < 20% or CCI < 7 on the results of the count made 1 to 24 hrs after a second transfusion of a concentrate of platelets: • Compatible ABO • Less than 48h of storage • Having a sufficient quantity of platelets (0.5 * 1011/7kg)
Non alloimmune Transfusional Storage Leucocytic contamination Clinics Fever splenomegaly CIVD . MAT CSH graft Immunological Auto antibody Immunoallergic antibodies Alloimmunes Anti-HLA Frequent Anti class I Anti-HPA Unknown frequency, probably weak Often not recognised Anti-AB Sometimes forgotten Causes of the refractory states to platelet transfusions
Study TRAP (Trial to Reduce Alloimmunization to Platelets Study Group N. Eng. J. Med. 1997) • Co-operative study 530 LAM • 4 groups of patients: • Transfused with pools of concentrates of normal platelets • Transfused with pools of concentrates of platelets treated with UV-B • Transfused with pools of concentrates of leucocyte-reduced platelets by filtration • Transfused with concentrates of platelets of apheresis with leucocytes reduced by filtration
TRAP study(Trial to Reduce Alloimmunization to Platelets Study Group N. Eng. J. Med. 1997) • Refractory state: • 2 consecutive ineffective transfusions,CCI in the hour following the transfusion < 5000/ L/m2 • Compatible ABO • At least one of the two concentrates stored for less than 48 hrs. • Anti-HLA • MLCT sensitized by an antiglobuline • 60% cytotoxicity in 1 cell or 40% in 2 • Tests prior to beginning of protocol and then every week for eight weeks • Anti-HPA • Detection: ELISA and flow cytometry • Confirmation: method of capture ELISA
TRAP Study (NR. Eng.J.Med. 1997)refractory states (RS) withtransfusions of platelets and alloimmunisation
Risk factors of alloimmunisation • Preliminary sensitizing • Previous blood transfusions without leucocyte reduction • Prevopis pregnancies 62% vs 33% of immunization with/without leucocyte reduction (TRAP study) • Pilot 32% vs 10% of immunization with products without leucocyte reduction vs products with leucocyte reduction (TRAP study)
Platelet transfusion What to do in the event of a refractory state? • search for AC anti HLA /HPA • Search for compatible platelets: phenotype CPA compatibilized cryostored • MCP
Platelet transfusion Other complications • Nonhemolytic feverish reactions • Anti-erythrocyte alloimmunization (rhesus) • Allergy • Haemolytic accidents (haemolysins) • GVHD • Transmission of viruses, bacteria, parasitic infectious diseases • TRALI • Post-transfusional purpura
Platelet transfusion Prevention of complications • RFNH: fresh platelets, deleucocytation, (deplasmatisation) premedication of the recipient • Alloimmunization anti D: Selection of platelets from Rh negative donor (protection future obstétrical +++)+++) Ig anti D Passive anti D monitoring • Allergy: Prefer additive platelets in solution to platelets in plasma, (deplasmatisation?)
Platelet transfusion • Haemolytic accidents (by AC immune ABO) Detection of haemolysins Respect Iso group if possible Plasma removal • GVHD Irradiation • Transmission of infectious diseases Tracking of viruses: HBV, HCV, HIV, MVC For the bacteria: medical maintenance, good disinfection of the intake point, rules of hygiene, information post donation
Platelet transfusion Transmission of infectious diseases (continued) For parasites: forty donors when returning from endemic areas Attenuation of pathogens: Amotosalen, Riboflavin, UVC, but deterioration of the platelet function involving of the more frequent transfusions
Platelet transfusion • TRALI • Not-transfused male subjects • Nulliparous women • Multiparous negative ac anti HLA
Post-transfusional purpura • Identification • Typical form of brutal thrombocytopenia one week after the transfusion of a blood product containing of the platelets • Atypical form: refractory thrombocytopenia with the transfusions of platelets • Diagnosis • In addition to frequently present anti HLA, look for anti-HPA interest of MAIPA with ac monoclonal suitable • Treatment • Generally ineffective transfusion since PR associates an anti HPA reaction automatically with an allo reaction • Plasma transplant • IVIG
Platelet transfusion Conclusion • Two products with identical effectiveness: CPA and MCP • Preserved in plasma or additive solution (PAS) • Able to use transformations or qualifications (phenotype, test of compatibility, negative CMV) to adapt to the needs of the patient • The selection, dose, and monitoring of platelet transfusions must be subject to dialogue between the prescriber and the transfusion centre
RemerciementsThanks • Pr. Jean-Yves Muller • Dr.Julie Vasse • Mme Soline Gaucheron • Mr Jean-Pierre Lebaudy • Distribution team