Download
1 / 84
850 likes | 1.99k Views
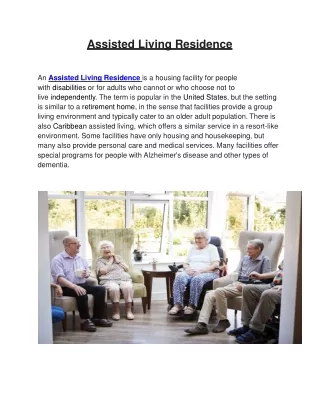
Skilled Care in Assisted Living Facilities. W. Tom Geary Jr. MD wt.geary@adph.state.al.us September 15, 2010. Skilled Care in the ALF/SCALF.

E N D
Skilled Care in Assisted Living Facilities W. Tom Geary Jr. MD wt.geary@adph.state.al.us September 15, 2010
Skilled Care in the ALF/SCALF • Skilled nursing care is health care given when a person needs skilled nursing staff (registered nurse (RN) or licensed practical nurse (LPN)) to manage, observe, and evaluate care. • Skilled nursing care requires the involvement of skilled nursing staff in order to be given safely and effectively.
Skilled Care in the ALF/SCALF “The goal of skilled nursing care is to help improve the patient's condition or to maintain the patient's condition and prevent it from getting worse.” Aetna Clinical Policy Bulletin:Skilled Home Health Care Nursing Services
Skilled Care in the ALF/SCALF “In determining whether a service requires the skills of a nurse, consider both the inherent complexity of the service, the condition of the patient and accepted standards of medical and nursing practice.” Information Bulletin 03-2 MHC-40 (for coverage of skilled home health services in Minnesota)
Skilled Care in the ALF/SCALF In Alabama: • Skilled nursing services are services rendered in accordance with the Alabama Nurse Practice Act (Code of Alabama, 1975, §§ 34-20 et. Seq.) and Alabama Administrative Code (Chapter 610) Alabama Board of Nursing. • Skilled Nursing services are provided pursuant to physician orders as part of a prescribed plan of care
Skilled Care in the ALF/SCALF • Alabama Board of Nursing Chapter 610-X-6 • Standards of Nursing Practice • (18) Assess individual competency when assigning selected components of nursing care to other health care workers including but not limited to: • (a) Knowledge, skills and experience. • (b) Complexity of assigned tasks. • (c) Health status of the patient. Author: Alabama Board of Nursing. Statutory Authority: Code of Alabama, 1975, §§ 34-21-2(c)(21), 34-21-25(b).
Skilled Care in the ALF/SCALF Nurses must exercise good judgment when assigning tasks to unlicensed personnel: • (4) Tasks delegated to unlicensed assistive personnel may not include tasks that require: • (a) The exercise of independent nursing judgment or intervention. • (b) Invasive or sterile procedures. (i) Finger sticks are not an invasive or sterile procedure within the meaning of these rules. (ii) Peripheral venous phlebotomy for laboratory analysis is not an invasive or sterile procedure within the meaning of these rules. • (c) The assistance with medications except as provided in Chapter 610-X-7. • (5) Supervision shall be provided to individuals to whom nursing functions or • responsibilities are delegated or assigned. • (6) The practice of licensed practical nursing shall be directed by a registered nurse • or physician or dentist. • (7) A licensed practical nurse or unlicensed individual may not supervise, direct, or evaluate the • nursing care provided by the registered nurse. Author: Alabama Board of Nursing Statutory Authority: Code of Alabama, 1975, §§ 34-21-1(3)(b), 34-21-2(a)(21), 34-21-2(c)(6). History: Filed November 23, 2009. Effective December 28, 2009. 610-X-4
Skilled Care in the ALF/SCALF 610-X-7-.06 Alabama Department of Mental Health Residential Community Programs (4) The specific delegated tasks shall not require the exercise of independent nursing judgment or intervention. Specific tasks that require independent nursing judgment or intervention that shall not be delegated include, but are not limited to: (a) Catheterization, clean or sterile. (b) Administration of injectable medications, with the exception of injectable medications for anaphylaxis such as the Epi-pen®. (c ) Calculation of medication dosages other than measuring a prescribed amount of liquid medication or breaking a scored tablet. (d ) Tracheotomy care, including suctioning. (e) Gastric tube insertion, replacement, or feedings. (f ) Invasive procedures or techniques. (g) Sterile procedures. (h) Ventilator care. (i) Receipt of verbal or telephone orders from a licensed prescriber.
Skilled Care in the ALF/SCALF ALF rules: 420-5-4-.06-(6)-(b) An assisted living facility shall not admit nor once admitted shall it retain a resident who requires medical or skilled nursing care for an acute condition or an exacerbation of a chronic condition which is expected to exceed 90 days unless:
Skilled Care in the ALF/SCALF • The individual is capable of performing and does perform all tasks related to his or her own care; OR (this means that the individual is at all times capable of and actually does perform all tasks related to the skilled need but may have a need for a professional to initiate and replace the device or process and provide the training and initial observations – for example: a Foley (bladder) catheter or implanted pain infusion pump)
Skilled Care in the ALF/SCALF 2. The individual is incapable of performing some or all tasks related to his or her own care due to limitations of mobility or dexterity BUT the individual has sufficient cognitive ability to direct his or her own care AND the individual is able to direct others and does direct others to provide the physical assistance needed to complete such tasks, AND the facility staff is capable of providing such assistance and does provide such assistance. (this includes limitation due to visual impairment)
Skilled Care in the ALF/SCALF The definition of what constitutes skilled care by any objective standard is constantly changing: it is a “moving target”. • In 1950 anyone would have been amazed to see a person with Lou Gehrig’s disease just using oxygen at home or in a boarding home. • Today it is not unusual to see such a person in their own home receiving skilled care for years with a tracheostomy on ventilator care!
Skilled Care in the ALF/SCALF • Many residents in assisted living use oxygen in association with a CPAP machine at night. As long as the resident can and does manage his or her CPAP and oxygen, this is acceptable. • By the same token, no one would claim that it is not skilled care requiring training and expertise to apply CPAP with oxygen to a person who can not provide any verbal feedback or directions regarding the process.
Skilled Care in the ALF/SCALF • We expect and allow the resident to use a mechanical nebulizer with appropriate medications for updraft treatments to control asthma or COPD. • But adding medication(s) to the nebulizer chamber and setting up the updraft equipment with a mask or oral inhaler for use by another person who can not direct the process is skilled nursing and/or skilled respiratory therapy care.
Skilled Care in the ALF/SCALF Since the administration of pulmonary medications by nebulizer is a medication administration issue, a licensed nurse may provide this delivery system in an ALF, or in a SCALF for residents who are cognitively unable to do this for themselves Unlicensed personnel can not manage the nebulizer treatments for residents who can not direct their own care.
Skilled Care in the ALF/SCALF • Some facilities have an automated defibrillator on the wall, similar to those in every airport, for use by non-professional personnel in the event of sudden cardiac arrest. • If any licensed health care facility has such a device we expect the staff to be trained in the use of the equipment.
Skilled Care in the ALF/SCALF • Some facilities have small, portable pulse-Ox oxygen saturation monitors for use by non-professional staff in obtaining vital signs. This is appropriate when coupled with the same degree of training and experience that is customary for nursing assistants in monitoring vital signs with blood pressure devices, thermometers, checking the heart rate, and training in what constitutes normal values and “panic” values for results.
Skilled Care in the ALF/SCALF • Allowing these sophisticated devices and procedures in the assisted living facility is surely a step forward. But this raises questions about other new processes and procedures:Why not allow anything in the ALF/SCALF if the FDA allows the equipment and/or the process in the home setting?
Skilled Care in the ALF/SCALF Home Health and Consumer Devices- Information from the FDA web site • FDA regulates medical devices that consumers use themselves without professional medical assistance in the same way as they regulate other medical devices. But the agency also focuses on how people can use these devices safely and effectively.
Skilled Care in the ALF/SCALF Risks such as infection or injury still exist with these products and everyone--FDA, the health professionals that prescribe the products, and consumers--have a role to play in prevention. Use in the assisted living means that the facility assumes a great deal of the responsibility for the safety and effectiveness of these products and devices.
Skilled Care in the ALF/SCALF • The FDA is also developing educational materials on the safe use of these devices. • There are no clear regulations for complex medical devices used in the home.
Skilled Care in the ALF/SCALF The CDC has targeted Assisted Living Facilities as a high risk area for transmission of Hepatitis B from the use of finger stick blood sugar monitors for multiple residents without disinfecting the glucometer itself after each use. MMWR March 11, 2005 / 54(09);220-223 Transmission of Hepatitis B Virus Among Persons Undergoing Blood Glucose Monitoring in Long-Term--Care Facilities --- Mississippi, North Carolina, and Los Angeles County, California, 2003—2004 Assisted Living Center B, Los Angeles County, California “Of the nine patients who had daily exposure to fingerstick procedures performed by nursing staff, eight had acute HBV infection, compared with none among the seven residents who performed their own fingersticks.”
BOX 1. Recommended practices for preventing patient-to-patient transmission of hepatitis viruses from diabetes-care procedures in long-term–care Settings A. Diabetes-care procedures and techniques • Prepare medications such as insulin in a centralized medication area; multidose insulin vials should be assigned to individual patients and labeled appropriately. • Never reuse needles, syringes, or lancets. • Restrict use of fingerstick capillary blood sampling devices to individual patients. • Consider using single-use lancets that permanently retract upon puncture. • Dispose of used fingerstick devices and lancets at the point of use in approved sharps containers. • Assign separate glucometers to individual patients. If a glucometer used for one patient must be reused for another patient, the device must be cleaned and disinfected. Glucometers and other environmental surfaces should be cleaned regularly and whenever contamination with blood or body fluids occurs or is suspected. • Store individual patient supplies and equipment, such as fingerstick devices and glucometers, within patient rooms when possible. • Keep trays or carts used to deliver medications or supplies to individual patients outside patient rooms. Do not carry supplies and medications in pockets. • Because of possible inadvertent contamination, unused supplies and medications taken to a patient’s bedside during fingerstick monitoring or insulin administration should not be used for another patient.
BOX 1. Recommended practices for preventing patient-to-patient transmission of hepatitis viruses from diabetes-care procedures in long-term–care Settings B. Hand hygiene and gloves • Wear gloves during fingerstick blood glucose monitoring, administration of insulin, and any other procedure involving potential exposure to blood or body fluids. • Change gloves between patient contacts and after every procedure that involves potential exposure to blood or body fluids, including fingerstick blood sampling. Discard gloves in appropriate receptacles. • Perform hand hygiene (i.e., hand washing with soap and water or use of an alcohol-based hand rub) immediately after removal of gloves and before touching other medical supplies intended for use on other patients.
BOX 2. Recommended medical management, training, and oversight measures to preventpatient-to-patient transmission of hepatitis viruses from diabetes-care procedures in longterm–care settings • Regularly review patient schedules for fingerstick blood glucose sampling and insulin administration and reduce the number of percutaneous procedures to the minimum necessary for appropriate medical management of diabetes and its complications. • Ensure that adequate staffing levels are maintained to perform all scheduled diabetes-care procedures, including fingerstick blood glucose monitoring. • Consider diagnosis of acute viral hepatitis infection in patients with illness that includes hepatic dysfunction or elevated liver transaminases (serum alanine aminotransferase and aspartate aminotransferase). • Provide a full hepatitis B vaccination series to all previously unvaccinated staff members with exposure to blood or body fluids. Check and document postvaccination titers 1–2 months after completion of the vaccination series. • Establish responsibility for oversight of infection control activities. Investigate and report any suspected case of newly acquired bloodborne infection. • Require staff members to know standard precautions and demonstrate proficiency in taking these precautions with procedures involving potential blood or body fluid exposures. • Provide staff members who perform percutaneous procedures with infection-control training that includes practical demonstration of aseptic techniques and instruction regarding reporting exposures or breaches. Conduct annual retraining of all staff members who perform procedures with exposure to blood or body fluids. • Assess compliance with infection-control recommendations (e.g., hand hygiene or glove changes) by periodic observation of staff and tracking use of supplies.
Skilled Care in the ALF/SCALF • The bureau recommends that glucometers be reserved for use by one individual. • Monitoring of blood sugars by finger-stick monitoring is skilled care. • The resident must be able to do all aspects of their own finger-stick blood sugar determination and interpretation - or have this performed by a nurse.
Skilled Care in the ALF/SCALF • However, there may be rare instances where the resident is cognitively intact but unable, due to limitations of mobility, dexterity, or vision, to perform his or her own fingerstick glucose determinations. If that resident is able at all times to direct the care assistant in all aspects of the physical assistance need to complete the procedure and the facility staff is capable of and does provide such assistance, the resident may remain in an assisted living facility without a nurse to perform the blood glucose determinations.
Skilled Care in the ALF/SCALF • Capable of providing the such assistance means that there is documentation that all facility staff/care assistants who assist the resident are: • Trained in performing finger-stick blood glucose determinations • Trained in the use, calibration, and maintenance of the glucometer • Educated, trained, and current with all the OSHA and CDC requirements for procedures which involve exposure to blood and body fluids
Skilled Care in the ALF/SCALF • Let’s look at a some examples of care interventions from the simple to the more complex.
Skilled Care in the ALF/SCALF 1. First Aid is not considered skilled care – the management of simple cuts, abrasions and skin tears; minor bug bites and stings, poison ivy exposure; minor burns; the Heimlich Maneuver; CPR
Skilled Care in the ALF/SCALF • First Aid may be rendered by an unlicensed person or by the resident to him/her self. • We require the staff to have training in CPR and expect them to perform CPR in the event of sudden unexpected cardiopulmonary arrest. • In the event of an emergency I would hope that even a visitor trained in first aid would come to the aid of anyone in acute distress.
March 2007 Talking About Disaster: Guide for Standard Messages First Aid Contents-1 • Produced by the American Red Cross • First Aid Kit Contents • *ACFAS MINIMUM RECOMMENDED FAMILY KIT CONTENTS • Assemble a first aid kit to include in your Disaster Supplies Kit and one for each vehicle. • Additional items may be added to personalize or customize this kit. • Family First Aid Kit Content Suggested Use • Absorbent Compress 5x9 dressing Cover and protect open wounds • Adhesive Bandages (Assorted Sizes) Cover and protect open wounds • Adhesive Tape (cloth) 1” To secure bandages or splints • Antibiotic Ointment packets (approx 1 g) Anti-infection • Antiseptic wipe Packets Wound cleaning/germ killer • Aspirin (Chewable) 81 mg For symptoms of a heart attack** • Blanket (Space Blanket) Maintain body temperature for shock • CPR Breathing Barrier (w/one-way valve) Protection during rescue breathing or CPR • Instant Cold Compress To control swelling • Gloves (large), disposable, non-latex Prevent body fluid contact • Hydrocortisone Ointment Packets (approx 1 g) External rash treatment • Scissors Cut tape, cloth, or bandages • Roller Bandage 3” (individually wrapped) Secure wound dressing in place • Roller Bandage 4” (individually wrapped) Secure wound dressing in place • Sterile Gauze Pad 3x3 To control external bleeding • Sterile Gauze Pad 4x4 To control external bleeding • Thermometer, Oral (Non-Mercury/Non-Glass) Take temperature orally • Triangular Bandage Sling or binder/splinting • Tweezers Remove splinters or ticks • First Aid Instruction booklet Self explanatory • *ACFAS is the American National Red Cross Advisory Council on First Aid and Safety
Workplace First Aid Cabinet for Food Services Industry Contents Include: • (2) 1" x 3" Visible Blue Bandage (25) Bandages • (1) Knuckle Visible Blue Bandage (20) Bandages • (1) Fingertip Visible Blue Bandage (20) Bandages • (5)2" x 2" Gauze Pads - Packs of 2 • (5)3" x 3" Gauze Pads - Packs of 2 • (1)2" Gauze Roll Bandage - 2" Roll • (1)1 3" Gauze Roll Bandage - 3" Roll • (1)Elastic Wrap Bandage - 2" x 5 yd. • (1)40" Triangular Sling/Bandage • (1)5" x 9" Trauma Pad • (20)Alcohol Cleansing Pad Pads • (20)Antiseptic Cleansing Wipe Wipes • (10)First Aid/Burn Cream Packs • (10)First Aid Antibiotic Ointment Packs • (6)Burn Relief Gel - 3.5 gm. Packs • (1)Eye Wash - 1 oz. Bottle • (10)Moleskin - 2" Squares • (1)CPR Face Shield paired with Gloves • (2)Pair of Vinyl Gloves • (1)First Aid Tape - 1/2" x10 yd. Roll • (1)Cloth First Aid Tape - 1" x 5 yd. Roll • (50)Bandage Protectant/Finger Cot • (1)Nickel Plated 4 1/2" Scissor • (1)Stainless Steel 3" Tweezer, Slanted • American Red Cross Emergency First Aid Guide
March 2007 Talking About Disaster: Guide for Standard Messages First Aid Contents-1 • Produced by the American Red Cross • First Aid Kit Contents • *ACFAS MINIMUM RECOMMENDED FAMILY KIT CONTENTS • Assemble a first aid kit to include in your Disaster Supplies Kit and one for each vehicle. • Additional items may be added to personalize or customize this kit. • Family First Aid Kit Content Suggested Use • Absorbent Compress 5x9 dressing Cover and protect open wounds • Adhesive Bandages (Assorted Sizes) Cover and protect open wounds • Adhesive Tape (cloth) 1” To secure bandages or splints • Antibiotic Ointment packets (approx 1 g) Anti-infection • Antiseptic wipe Packets Wound cleaning/germ killer • Aspirin (Chewable) 81 mg For symptoms of a heart attack** • Blanket (Space Blanket) Maintain body temperature for shock • CPR Breathing Barrier (w/one-way valve) Protection during rescue breathing or CPR • Instant Cold Compress To control swelling • Gloves (large), disposable, non-latex Prevent body fluid contact • Hydrocortisone Ointment Packets (approx 1 g) External rash treatment • Scissors Cut tape, cloth, or bandages • Roller Bandage 3” (individually wrapped) Secure wound dressing in place • Roller Bandage 4” (individually wrapped) Secure wound dressing in place • Sterile Gauze Pad 3x3 To control external bleeding • Sterile Gauze Pad 4x4 To control external bleeding • Thermometer, Oral (Non-Mercury/Non-Glass) Take temperature orally • Triangular Bandage Sling or binder/splinting • Tweezers Remove splinters or ticks • First Aid Instruction booklet Self explanatory • *ACFAS is the American National Red Cross Advisory Council on First Aid and Safety
Skilled Care in the ALF/SCALF Once the treatment is beyond First Aid --and usually by this time the physician is involved-- there must be a licensed nurse providing all skilled care including the supervision of dressings and any other treatments. • Care assistants may provide and assist with application of ice/cold packs for residents who have a sprain or minor joint pain. • Care assistants may not provide or apply hot packs due to concern for burns in the elderly. • Residents who are cognitively intact may use their own heating pad.
Skilled Care in the ALF/SCALF 2. Wound care and dressing changes. Nurses (RN or LPN) in the ALF or SCALF can apply dressings as ordered with or without topical medication(s) for a skin injury such as a skin tear or scrape, or a laceration, a surgical wound, or a small pressure ulcer. All of these conditions are expected to resolve in less than 90 days. This may be the facility nurse or the Home Health nurse.
Skilled Care in the ALF/SCALF If a wound fails to heal in 60 days, the facility must give the resident and sponsor a 30 day discharge notice. It could still heal at day 89 – but its not very likely. It is obvious that something more significant is going on when a wound is not healing in 60 days. In those situations a higher level of care is needed for further assessment of the wound and the overall physiologic status of the resident.
Skilled Care in the ALF/SCALF • Wound care involves much more that just removing and reapplying the dressing every day or every few days. • Comprehensive Wound Assessment and Care involves: Assessing the character of the tissue, drainage, necrosis and infection in the wound base, tunneling, status of the surrounding skin (integrity, infection); circulation; concurrent medical conditions; effects of medication; nutrition; activity
Skilled Care in the ALF/SCALF • All of these parameters are important to the process and require specialized training for nurses (Beyond Basic Training). • Why can’t the Home Health nurse who is a certified WOCN be the one to provide comprehensive wound care beyond 90 days in the ALF or SCALF? • No ALF or SCALF facility is staffed with full-time, professionally trained personnel from each discipline to provide this level of integrated care and oversight.
Skilled Care in the ALF/SCALF There are many specialized mechanical devices which are marketed to assist in wound healing and are applied to wounds continuously to: • Negative pressure wound care • Electronic current therapies • Sequential intermittent pneumatic compression (IPC) device All of these have potential serious side effects and require continuous trained personnel for monitoring and represent skilled care that is inappropriate in the ALF/SCALF.
Skilled Care in the ALF/SCALF • Intermittent wound therapies that are applied early in the care of a wound ( <90 days) during a visit by the Home Health Nurse and removed at the time the nurse leaves are acceptable in the ALF or SCALF. • Examples: LED laser light therapy, MIRE (Monochromatic InfraredEnergy) at the specific wave length of 890 nm, Hydrotherapy
Skilled Care in the ALF/SCALF 3. What about pulsed electromagnetic devices for bone healing in nonunion fractures? • Currently, a number of electrical bone growth stimulators (EBGS) devices and ultrasound devices have been approved by the FDA for treating nonunion fractures. • The noninvasive EBGS are portable, battery operated devices applied to the area for as long as 12-24 hours daily.
Skilled Care in the ALF/SCALF These devices are acceptable in the ALF or SCALF as an aid to healing of fractures and return to normal mobility. In the SCALF there may be few residents who would benefit from such therapy and who could tolerate this without becoming noncompliant with such a device attached to a limb for hours and hours every day for weeks. Overall, EBGS is considered safe and well tolerated. No major side effects or complications have been reported in the literature.
Skilled Care in the ALF/SCALF 4. Ostomy Care This type of care can be safely done by any alert and mentally intact person who is intellectually and emotionally willing and able to learn how to manage his or her own ostomy. The teaching is done by a nurse specially trained in wound and ostomy therapy (WOCN).
Skilled Care in the ALF/SCALF • In the setting of the hospital, home health, and nursing home, only nurses with training and experience care for ostomies. • Nursing assistants, CNA’s, family members, and sitters never provide ostomy care in any licensed health care setting.
Skilled Care in the ALF/SCALF • If a resident is able to provide all of his/her own ostomy care, that person is acceptable for assisted living. If the resident can and does direct the staff who are trained in ostomy care to do all the care, that resident may remain in assisted living. • If that residentbecomes unable to provide all of their own care or, because of cognitive decline they become unable to continuously direct and monitor the care for their ostomy, that person is no longer appropriate for any assisted living facility.
Skilled Care in the ALF/SCALF • The care assistants must have training in the infection control aspects of ostomy care as well as the mechanics of performing ostomy bag changes. The resident must continue to provide all of the technical assessment of the site and the function of the ostomy and be able to report any problems with the function of the ostomy.
Skilled Care in the ALF/SCALF 5. Urinary Catheter Bladder catheter management requires skilled nursing care to insert and change the catheter. If the resident in a regular ALF is able to manage the catheter and the tubing and the urine bag – then there is not a problem with home health nurses providing intermittent skilled care beyond 90 days to change the catheter or obtain the occasional urine culture.
Skilled Care in the ALF/SCALF If a resident is unable, for whatever reason, to understand how to manage the catheter and tubing that resident is ineligible for assisted living. For example, the resident is constantly pulling on the catheter causing bladder irritation, or is contaminating the building with a leaking catheter bag, or is unable to understand that back-flow of cloudy urine into the bladder and a twisted and obstructed catheter represent major infection risk factors.
Skilled Care in the ALF/SCALF • Condom Urinary catheters for male residents: The care and management of condom catheters requires training and experience. If a resident is capable of applying and managing his own catheter, this is acceptable in an assisted living facility.