Download
1 / 25
250 likes | 400 Views
Beyond Front-line Sunitinib in Metastatic RCC. Brian I. Rini, M.D. Department of Solid Tumor Oncology Cleveland Clinic Taussig Cancer Center. Sunitinib as front-line Why/when do we stop sunitinib? What do we do next (mTOR vs. VEGF)? Clinical options Sunitinib rechallenge Axitinib.

E N D
Beyond Front-line Sunitinib in Metastatic RCC Brian I. Rini, M.D. Department of Solid Tumor Oncology Cleveland Clinic Taussig Cancer Center
Sunitinib as front-line • Why/when do we stop sunitinib? • What do we do next (mTOR vs. VEGF)? • Clinical options • Sunitinib rechallenge • Axitinib
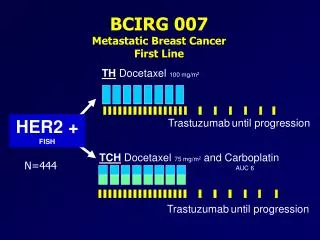
Best Response by RECIST (Independent Central Review) ** Sunitinib vs IFN-α: p <0.000001
Sunitinib vs. Interferon in untreated metastatic RCC: PFS 1.0 0.9 0.8 Median progression-free survival: 0.7 Sunitinib = 11.0 months 0.6 IFN- = 5.1 months Progression-free survival probability 0.5 0.4 Hazard Ratio=0.538p < 0.000001 0.3 0.2 0.1 0.0 0 5 10 15 20 25 30 Time (months)
Final Overall Survival Total Death Sunitinib 190 IFN-a 200
RECIST oftenisinadequate treatment Abou-Alfa G, et al. EORTC-NCI-AACR 2004, Geneva, Switzerland
Patterns of tumor progression on VEGF or VEGFR inhibitors Change in TumorMeasurements (%) Change in TumorMeasurements (%) Change in TumorMeasurements (%) Primary refractory Early progressors Late progressors
Baseline s/p 2 cycles sunitinib 50 mg s/p 4 cycles sunitinib37.5 mg s/p 2 cycles sunitinib50 mg
Disease progression, including new metastases, clinically involves enhanced perfusion (i.e. VEGF-driven angiogenesis) Pre-TKI = -22d Post-TKI = 53d Pre-Prog = 467d Prog = 556d RP Liver New Metastases Slide courtesy of Shetal Shah, MD CCF
Time to Treatment Failure: from second-line drug initiation (n=216) Vickers et al. Urology 2010
2nd-line VEGF vs. mTOR • Adjusting for MSKCC prognostic profile, the hazard ratio for TTF was 0.5 (95% CI:0.29-0.91) in patients receiving anti-VEGF therapy • Adjusting for non-clear cell histology and sarcomatoid features, the statistical difference in favor of VEGF-targeted agents persisted (HR 0.5, 95% CI: 0.27-0.9) • Overall survival (OS) from start of 2nd-line therapy: anti-VEGF vs. anti-mTOR therapy (14.2 vs 10.6 mos; p=0.38)
Results in VEGF-targeted Therapy-refractory RCC Patients * Clinical activity is greatest with drugs that more potently inhibit VEGF-R * More modest clinical effect is seen with mTOR inhibition in this setting, similar to weak VEGF-R inhibition
Clinical Activity of Sunitinib Rechallenge in Metastatic Renal Cell Carcinoma B. I. Rini1, T. E. Hutson2, P. Elson1, D. Y. C. Heng3, J. J. Knox4, D. M. Michaelson5, T. K. Choueiri6, B. Escudier7 • Cleveland Clinic Taussig Cancer Institute, Cleveland, OH • Texas Oncology / Baylor Sammons Cancer Center, Dallas, TX • Tom Baker Cancer Centre, University of Calgary, Calgary, AB • Princess Margaret Hospital, Toronto, ON • Massachusetts General Hospital, Boston, MA • Dana-Farber Cancer Institute, Boston, MA • Institut Gustave Roussy, Villejuif, France
Results • The median PFS of initial treatment with sunitinib was 13.7 months compared to 7.2 months for rechallenge (p=0.04) • The PFS was longer with rechallenge than with initial treatment in 6 patients (26%) • Patients with a > 6 month duration between sunitinib treatments had a longer PFS than patients who were rechallenged within 6 months. • median PFS 16.5 vs. 6.0 months; p=0.03 • There was no significant difference in outcome to sunitinib rechallenge based on number or type of intervening treatments
Relative Potencies of TKIs in RCC 1. Eskens FALM, et al. In: Proceedings of the 99th Annual Meeting of the AACR. San Diego, CA: AACR; 2008. Abstract LB-201. 2. Nakamura K, et al. Cancer Res. 2006;66(18):9134-9142. 3. Chow LQM, Eckhardt SG. J Clin Oncol. 2007;25(7):884-896.
Axitinib in cytokine-refractory RCC • In an intention-to-treat analysis, two complete and 21 partial responses were noted, for an objective response rate of 44.2% (95% CI 30·5–58·7). • Median response duration was 23.0 months (20·9–not estimable; range 4·2–29·8). • Median time to progression was15.7 months (8·4–23·4, range 0·03–31·5) and median overall survival was 29.9 months (20·3–not estimable; range 2·4–35·8). Rixe et al. Lancet Oncology 8 (11), 2007
Axitinib in sorafenib-refractory RCC: Baseline Characteristics
Best Response by RECIST *1/14 patients who had prior sorafenib and sunitinib treatment had a PR **9/14 patients who had prior sorafenib and sunitinib treatment had tumor shrinkage
Conclusions • Sunitinib is a front-line standard of care. • Determination of progression on sunitinib (meaning no further clinical benefit) is often difficult. • RCC is a VEGF-driven disease, and remains so during and after progression on VEGF suppressive (e.g. sunitinib) therapy. • The most robust clinical results in VEGF-refractory RCC correlate with continued VEGF targeting (even sunitinib again) and potency against the VEGF receptor (e.g. axitinib).