Download
1 / 55
760 likes | 1.42k Views
Review of Current Intraosseous Infusion Devices. Lecture Outline. Review relevant anatomy, indications, & contraindications Present background reasons for interest in expanding use of intraosseous (IO) line insertion in adults

E N D
Lecture Outline • Review relevant anatomy, indications, & contraindications • Present background reasons for interest in expanding use of intraosseous (IO) line insertion in adults • Describe the insertion procedure for the 4 types of currently approved IO devices
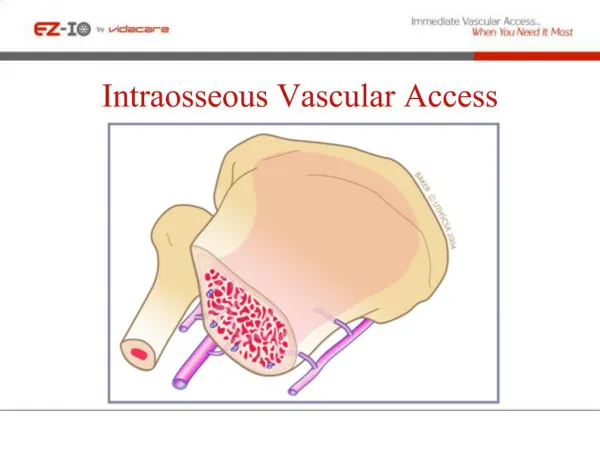
Relevant Anatomy Thousands of small veins lead from the bone medullary space to the general circulation
Intraosseous (IO) Pressure and Flow Rates • With a pressure bag or IV pump, Intraosseous (IO) flow rates are similar to IV’s through a 21-gauge needle. • Rate of infusion that can be given IO under 300 mm pressure : • 2 to 50 cc / min (average 10 cc / min) • 120 to 3,000 cc / hour (average 600 cc / hour) • Unit of blood in about 30 minutes • Rate of infusion that can be given IO under 1 meter gravity: • 1 to 15 cc / min (average 4 cc / min) • Unit of blood in about 60 minutes • Unit dose injections can be given in seconds (5cc in 3 sec) • Rapid 10 cc syringe bolus dramatically increases IO flow rates If no flush ---- there may be no flow !
IO Infusion of Medication • Which Drugs can be given ? • Any medications that can be safely injected into a peripheral IV can likewise be safely injected IO • Caution with cytotoxic drugs and hypertonic saline • What Dose ? • IO medication doses are the same as those for IV injection • Flow rates (Rapid 10 cc bolus must be given first) : • To maintain optimal flow, pressure of 300 mm Hg must be applied to the infusion bag or the pump • Testing : • 5 cc of blood can be aspirated from an IO device and placed into a heparin-coated syringe for standard laboratory testing
Potential IO Complications • Extravasation (leakage) • Dislodgement • Compartment syndrome • Fracture of the bone • Failure • Pain (more about this on next slide) • Infection • Experience in thousands of children and reports on 4,000 adults show the infection rate to be less than 0.6 % and those infections are usually not serious (can be treated as outpatients with removal of device) Mortality from above complications : None
Pain from IO Insertion • 85 % of IO patients will be unconscious • For them, pain is not an issue • For the conscious patient : pain is an issue • Pain related to insertion of needle : Minimal • May numb the skin and periosteum with local xylocaine • Pain related to infusion of meds / fluids (visceral pressure) • Numb the vessels by injecting xylocaine 10 mg IO • Psychological anxiety : “You are going to do what ?” • Talk to your patient first
Two Kinds of Pain Related to IO Insertion
IO Contraindications • Local Infection • Major trauma to extremity : fractures in same limb • Prosthesis • Recent (24 hours) previous IO • Vascular compromise : diabetic leg (relative contraindication) • Absence of anatomical landmarks • Osteogenesis Imperfecta
IO Indications • Cardiac arrest • Status epilepticus • Shock / Trauma • Arrhythmia • Dehydration • Burns • Drug overdose • DKA (diabetic) • End stage renal disease • Stroke • Myocardial infarction • Coma • Head Injury • Anaphylaxis • Congestive heart failure • Dialysis • Emphysema • Respiratory arrest • Hemophiliac crisis • Sickle Cell crisis • Pediatric shock • Chest pain IV access is often difficult or impossible in these situations. IO is the Answer !
Anatomic Sites for IO Insertion • Just below and medial to tibial tubercle (preferred site for both children and adults) • Lower anterior femur (for children) • Alternative sites for adults : • Ankle medial malleolus • Anterior humeral head • Sternum • Patella
Current IO State-of-the-Art • Universally taught as a core skill to : • Paramedics • Emergency physicians • Emergency and Pediatric Nurses • Used as a rescue IV access port in pediatrics • Current Standard of Care for children • So far only used sporadically in adults • New groundswell of interest for adults in past year • New ACLS, PALS, ATLS, ENPC guidelines recommend adult IO for difficult vascular access
The IO Paradigm is Changing • No adult devices :New adult IO devices have been FDA approved. • Fear :15 years experience in children has dispelled the fear of penetrating someone’s bone. • Infection :Infection has not been a problem. • Pain :Pain is controllable. • Difficult :New devices make the procedure easier than starting an IV. • No Support :Strong support from military, EMS, ER, ACLS. • Now the “Standard of Care” : PALS, ACLS, Military .
New IO Mandate “The use of IO devices is a promising technique to establish emergency access in adult patients” . American Heart Association : 2003 ACLS Principles & Practice
IV’s Are Difficult in Military Situations • Battlefield conditions • Darkness with use of night vision equipment • Hot or cold environments • Stressful : bullets flying overhead • Ratio of medics to troops : 1 to 40 or higher • Medic has to carry everything he needs in his rucksack (50 kg limit) • Training & experience • Medics are generally well trained • But have little opportunity for experience until actually needed • Is civilian prehospital trauma care any different ? • IV’s are just as difficult • Many of the same factors apply
Unnecessary Deaths • Acute hemorrhage is the major cause of Battlefield Mortality • 50 % are killed immediately • 50 % die within 1 hour of injury • Improvement in care requires • Control of bleeding • Rapid IV administration of blood & fluids • Most serious casualties go into shock • Veins collapse making IV access difficult • Average time for a medic to start an IV = 12 minutes • Average success rate in battlefield conditions = 30 % For 10 casualties it could take 2 hours to start IV’s
National Academy of Sciences Institute of Medicine, 1999
F.D.A. Approved IO Devices • Jamshidi / Illinois Sternal / Cook (manually pushed in) needles • Mostly used for pediatrics • F.A.S.T. Pyng (Bed of Nails) • Designed for adult sternum • Manually inserts 10 needles at once • B.I.G. Bone Injection Gun (Nail Gun) • Shoots a needle into adult tibia and other bones • EZ-IO (Battery Powered Drill) by VidaCare Company • Powers a hollow drill (Catheter) into the medullary space
Manually Inserted IO Needles Manually inserted hand held infusion needles have been available for years. Mostly used for infants because their bones are soft.
F.A.S.T. Insertion Procedure Do not attempt to use the F.A.S.T. 1 system unless you have been formally trained, evaluated, and authorized to perform this procedure !
F.A.S.T. Insertion Procedure • Undo or cut shirt to expose sternum. • Prepare the area of the manubrium with the iodine and alcohol swabs included in the package : wipe the area 1” below the sternal notch.
F.A.S.T. Insertion Procedure • Remove top half of backing labeled 1. • Place index finger in patient’s sternal notch ; the locating finger must be perpendicular to the manubrium. • Align Patch notch with patient’s sternal notch.
F.A.S.T. Insertion Procedure • Reaching under the Patch, remove backing labeled 2 and press Patch to skin. • Secure first half of the patch by pressing firmly downward, engaging the adhesive.
F.A.S.T. Insertion Procedure • Verify location : check that the locating notch matches the sternal notch and that the Target Zone is over the manubrium. • This is critical for safe and effective placement of the device.
F.A.S.T. Insertion Procedure • Remove Sharps Cap from the introducer ; the clear plastic Sharp Cap can be removed by slightly twisting and pulling away. • Place the bone probe cluster in the target zone with its long axis PERPENDICULAR (90 DEGREES) TO THE SKIN. • Ensure needle cluster is within the target zone.
F.A.S.T. Insertion Procedure • Press the Introducer into the target zone with firm and increasing force, until a distinct release of the Introducer handle is heard and felt. • The force must be applied in line with the long axis of the Introducer ; the forearm and elbow must be in line with Introducer’s axis. • After release pull straight back to remove the Introducer. 14 15
F.A.S.T. Insertion Procedure 16. Attach the right-angle female connector to the infusion tube. 17 • Attach syringe to straight female connector and withdraw marrow into the Infusion Tube to verify successful placement. • Remove and discard syringe. 18
F.A.S.T. Insertion Procedure Place the protector dome over the patch and press down firmly to engage the velcro fastening. 19.
F.A.S.T. Removal Procedure • Remove the Protector Dome from the Target Patch. • Disconnect the Infusion Tube from the right angle female connector on the Patch. Do not pull on the infusion tube to remove it ! 20 21
F.A.S.T. Removal Procedure (Continued) 1 • Insert the Remover into the Infusion Tube : keep the Infusion Tube straight out (90 degrees) from the patient. • Advance the remover till you hear or feel it enter the threads in the proximal tip of the infusion tube. • Turn the remover clockwise until it stops. • Pull straight out on the remover to remove the infusion tube. 2 3 4
The B.I.G™ IO Device Pediatric B.I.G : 18 Gauge FDA Approved Adult B.I.G : 15 Gauge FDA Approved
B.I.G. Technique of Insertion Use a povidone iodine tincture sponge to clean the selected site for injection. Position the front of the B.I.G™ at the selected site, holding and pushing firmly on the rear of the instrument.
B.I.G. Insertion Sequence 1 . 4 2 5 3
B.I.G. Technique of Insertion Position the BIG with one hand to the site and pull out the Safety Latch with the other hand.
B.I.G. Technique of insertion Trigger the BIG at 90º to the surface.
B.I.G. Technique of Insertion Remove the BIG. Pull out the stylet (trocar).
Technique of insertion Connect IV Set with a stopcockand flush with 1 mg / kg for IO local anesthetics. Fix the cannula with the Safety Latch.
The “EZ-IO” Drill Device “Making difficult IV access a thing of the past” Jointly owned and developed by The University of Texas Health Science Center & VidaCare Corporation
Univ. of Texas in San Antonio . Dr. Larry Miller who developed the EZ-IO device
EZ-IO Description • Establishes IO access simply & automatically • Uses a hollow drill to enter the bone • Small battery powered driver implants the needle • Enables immediate access for all drugs and fluids • Provides safe and easy IO access for adults “A kinder - gentler way”
Final Design EZ-IO needle and sheath The EZ-IO drill
How Adult EZ-IO Infusion BenefitsEmergency Medicine • Saves time • Takes less than 10 seconds • IV’s take an average of 8 minutes • One provider can treat multiple patients (Mass casualties) • Faster transport (less time on scene) • Improves throughput time (in the emergency department) • Can be started en route (less scene time) • Allows provider to handle other problems : i.e. airway, meds