Download
1 / 20
200 likes | 502 Views
The Analysis of Brain Lesions in Neuropsychiatric Systemic Lupus Erythematosis. H Jeremy Bockholt Charles Gasparovic The MIND Institute / UNM Albuquerque, NM NA-MIC All Hands Meeting 20070111 Salt Lake City, Utah. Background and Significance.

E N D
The Analysis of Brain Lesions in Neuropsychiatric Systemic Lupus Erythematosis H Jeremy Bockholt Charles Gasparovic The MIND Institute / UNM Albuquerque, NM NA-MIC All Hands Meeting 20070111 Salt Lake City, Utah
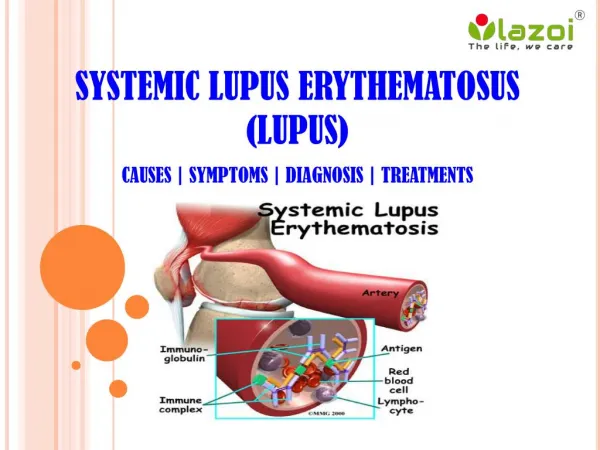
Background and Significance • Systemic lupus erythematosus (SLE) is an autoimmune disease affecting multiple tissues, including the brain • the facial rash of some people with lupus looked like the bite or scratch of a wolf ("lupus" is Latin for wolf and "erythematosus" is Latin for red). patients may feel weak and fatigued, have muscle aches, loss of appetite, swollen glands, and hair loss, sometimes have abdominal pain, nausea, diarrhea, and vomiting. • Estimates of SLE prevalence range from 14.6-372 per 105 • About 1.5 million americans, 90% diagnosed are female • Neuropsychiatric SLE (NPSLE), a term that subsumes the neurologic and psychiatric complications of SLE, occurs in up to 95% of SLE patients • While MRI often reveals distinct white matter abnormalities in active NPSLE, the pathologic processes underlying these lesions, whether purely autoimmune or vascular (e.g., hemostasis), are unknown
Aims of the RO1 Study • Test hypotheses concerning the possible thrombotic or embolic origin of white matter brain lesions in NPSLE • Examine whether the incidence of lesions correlates with either levels of thrombosis markers or emboli in the blood or a potential source of emboli in the heart • Examine whether overall lesion load or the levels of particular classes of lesion correlate with cognitive function
Background and Objective • Critical to understanding the etiology of brain lesions in NPSLE will be the accurate measurement of their location, size, and time course. • Lupus brain lesions are known to vary in MRI intensity and temporal evolution and include acute, chronic, and resolving cases. • Monitoring the time course of image intensity changes in the vicinity of lesions, therefore, may serve to classify them based on their temporal characteristics. • Major objective of this DBP will be the evaluation of existing tools and the development new tools using the NA-MIC kit for the time series analysis of brain lesions in lupus.
Summary of MRI Protocol • The MRI data in this project are collected on a 1.5T Siemens Sonata scanner using an 8-channel head coil. • T1-weighted 3D fast low angle shot (FLASH) sequence (TR/TE = 12/4.76ms, flip angle = 20deg, FOV = 220x220mm, resolution = 192x192, 120 1.5-mm slices, total time = 6m32s) • T2-weighted fast spin echo sequence (TR/TE = 9040/64ms, turbofactor=5, FOV = 220x220mm, resolution = 192x192, 120 1.5-mm slices, total time = 6m2s) • Fluid Attenuated Inversion Recovery (FLAIR)/fast spin echo sequence (TR/TE = 1000/105ms, TI = 2500ms, echo train=9, field of view (FOV) = 220x220mm, resolution = 192x192, 88 1.5-mm slices, total time = 9m2s).
Additional Protocol • transcranial doppler ultrasound is used to detect microemboli in the brain • transesophageal echocardiography is performed to evaluate general cardiac status and to detect the presence of heart valve vegetations, as potential sources of emboli. • markers of hemostasis, • analyses for platelets, coagulation, fibrinolysis, and anti-phospholipid antibodies. • battery of neuropsychological tests is administered to evaluate cognitive function.
Summary of Study Design • Clinical Assessments and MRI will be performed on approximately 60 SLE patients and 30 normal control subjects over a period of 48 months. • Subset of this group will be approximately 15 SLE subjects with NPSLE and 15 SLE subjects without NSLE • Subset of initial SLE groups will be re-examined in the each of the subsequent years (2-4) of the study.
Image Processing Needs • Co-registration of T1, T2, and FLAIR. • A robust and reliable method capable of segmenting the brain into at least four classes: gray matter, white matter, cerebrospinal fluid, and white matter lesions. • Longitudinal follow-up registration • Correlations such as appearance of and changes in particular lesions correlate with the onset and remission of the neuropsychiatric symptoms of NPSLE. • Others to be pointed out during discussion and perhaps ones that we do not even know about yet
Goals of the NPSLE DBP • Use and extend the NA-MIC kit to make a fully automated lesion analysis tool. • Input data • image data from the T1-weighted, T2-weighted, and FLAIR sequences • Output data • will be probability maps for each tissue class, the number of lesions, the volume of each lesion, and the total lesion volume at each time point • Changes in lesion size and changes in pixel intensity within the volume of each lesion will be displayed graphically • Time course data will also be amenable to time series analysis by statistical tools such as general linear modeling (GLM), independent component analysis (ICA), or potentially Bayesian analysis
Example NPSLE Lesion Hypointense on T1 Hyperintense T2 Hyperintense on FLAIR
TMI/UNM Current Tool Use • A number of different MRI data analysis tools are used by researchers at TMI and UNM: • Slicer • Mutli-modal Scientific Visualization • BRAINS2, FSL, SPM, Freesurfer, and Slicer • for image segmentation and labeling • FSL, SPM, and AFNI • used fMRI data analysis • GTRACT, DTIStudio • Used for DTI/DWI analysis
Goals Aug 2007 - July 2008 • Collect Baseline data points • Hire experienced C++ programmer, train and mentor to become expert at using NA-MIC kit • Evaluate the algorithm/approach performance of at least four methods for lesion segmentation of NPSLE brain images: • EM-Segment Method, developed by Sandy Wells • Modification of EM-Segment, developed by Vincent Magnotta • K-means+discriminant analysis, developed by Vincent Magnotta • Manual classification by an expert rater. We will use the STAPLE and/or a method using the Williams Index to cross-validate these methods.
Goals Aug 2008 - July 2009 • Complete collection of follow-up data points • Participate in the overall NA-MIC grant renewal process • Use and extend the NA-MIC kit to develop a lesion analysis module that provides a workflow for the registration of T1,T2, and FLAIR within and across different scanning sessions, automated segmentation into gray, white csf, and lesion, and summary of lesion location, size, and intensity. A fully-functional prototype will be completed in time for grant resubmission. • Extend lesion analysis module to provide time series analysis tools as the follow-up data points become available
Goals Aug 2009 - July 2010 • Complete a final, stable production time series lesion analysis module to be made available in NA-MIC kit • Provide final publically available data-sets to support a robust training tool for using the module • Contingent on renewal funds, try out different statistical methods of time series analysis, drawing from methods that have been successful in the analysis of fMRI data, including GLM and ICA • Use GLM or multiple regression analysis to examine correlations between changes in lesion intensity or size and measures of thrombo-embolic activity or the onset of clinical symptoms of NPSLE
NPSLE DBP Driving Force • Methods developed in this DBP will have a broad impact on the study of brain diseases involving MRI-visible lesions • Characterization of the time evolution of these lesions will undoubtedly help to elucidate not only the origins of the lesions but their relationships to disease symptoms. • No current image analysis package currently permits this level of automated lesion time series analysis--this will make the NA-MIC kit unique and more desirable to be used by the broader community
NPSLE DBP Summary • Using the NA-MIC kit, we will augment, develop, and validate tools for the quantification of brain lesions thought to underlie the cognitive dysfunction of NPSLE. • We will extend NA-MIC kit to analyze changes in these lesions with time and to relate these changes to the fluctuating symptoms of NPSLE • We will gain greater insight of NPSLE etiology • The automated lesion time series analyses should generalize well to other vascular disorders such as vascular dementia, myotonic dystrophy, and multiple sclerosis.
The MIND Institute / UNMThe Analysis of Brain Lesions in Neuropsychiatric Systemic Lupus Erythematosis INVESTIGATORS: H. Jeremy Bockholt Charles Gasparovic, Ph.D. CONSULTANTS: Vincent Magnotta, Ph.D. Vince Calhoun, Ph.D. PROGRAMMER: Sumner Williams, M.S. BACKGROUND: • NPSLE is an autoimmune disorder that causes neurological and psychiatric complications • Afflicted patients have distinct white matter lesions that vary over time • To understand the etiology of brain lesions in NPSLE, accurate measurement of lesion location, size, and time course must be achieved • AIMS: • Evaluate existing tools and develop new tools using the NA-MIC kit for time series analysis of brain lesions found in NPSLE DATA: • MRI, DTI, perfusion, transcranial ultrasound, echocardiography, and neuropsychology Data collected under R01-NS35708-04
References 1. Aladjem, H (Editor): LFA study shows between 1,400,000 and 2,000,000 people diagnosed with lupus. Lupus News 14:12, 1994. • Sibbitt WL Jr, Brandt JR, Johnson CR, Maldonado ME, Patel SR, Ford CC, Bankhurst, AD, BrooksWM: The incidence and prevalence of neuropsychiatric syndromes in pediatric-onset systemic lupus erythematosus. J Rheum 2002 29:1536-42. • Warfield SK, Zou KH, Wells WM. Simultaneous truth and performance level estimation (STAPLE): an algorithm for the validation of image segmentation. IEEE Trans Med Imaging. 2004 Jul;23(7):903-21. 4. Martin-Fernandez M, Bouix S, Ungar L, McCarley RW, Shenton ME. Two methods for validating brain tissue classifiers. Med Image Comput Comput Assist Interv Int Conf Med Image Comput Comput Assist Interv. 2005;8(Pt 1):515-22.
Acknowledgements • Charles Gasparovic • Wilber Sibbit • Carlos Roldan • Bruce Rosen • John Rasure • DOE Grant No. DE-FG02-99ER62764 • Function BIRN • Lupus: R01-NS35708-04
Questions and Discussion • Preprocessing and filtering • Baseline Shape Analysis • Longitudinal Change Shape Analysis • Anatomical Localization of Lesions • Longitudinal Matchup of Lesions • Is the timeline reasonable? • Should we extend and generalize the EM Segment Module or develop a standalone module? • Other items and discussion?