Download
1 / 26
290 likes | 591 Views
Endocarditis Pericarditis. EKG Changes indicative of Disease Processes other than STEMI. Bundle of His. Janeway lesions are seen in people with acute bacterial endocarditis. They appear as flat, painless, red to bluish-red spots on the palms and soles.

E N D
Endocarditis Pericarditis EKG Changes indicative of Disease Processes other than STEMI
Janeway lesions are seen in people with acute bacterial endocarditis. They appear as flat, painless, red to bluish-red spots on the palms and soles.
Osler’s nodes and splinter hemorrhages (longitudinal streaks in nail).
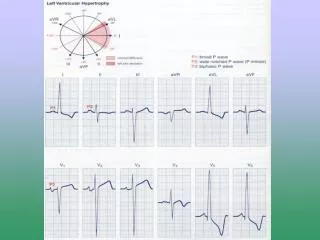
Sinus tachycardia PR depression ST elevation
Common Causes of Infectious Pericarditis Bacteria Haemophilus influenzae Mycobacterium Neisseria gonorrhoeae Neisseria meningitidis Salmonella Staphylococcus aureus Streptococcus pneumoniae Virus Coxsackievirus A and B Echovirus Epstein-Barr virus HIV Influenza virus Paramyxovirus Parvovirus B19 Fungi Aspergillus Blastomyces Candida Coccidioides immitis Cryptococcus neoformans Histoplasma capsulatum
PR depression is seen in the early phase of pericarditis and is followed by changes such as: ST segment elevation Normalization of the ST segment T-wave inversion Normalization of all changes over several days to weeks Low-voltage complexes are seen in pericarditis with pericardial effusion.
In patients diagnosed with an infectious disease, electrocardiography can be used to evaluate for cardiac involvement, provide information on prognosis, and assess the effect of treatment. Abnormalities on the electrocardiogram (ECG) of a febrile patient in whom late-stage Lyme disease is suspected can point to the diagnosis; conduction and rhythm disturbances are the most common ECG findings. In a patient with known endocarditis and persistent fever despite appropriate therapy, heart block on repeated ECG may indicate the presence of complicated valve abscess.
Myocarditis is caused by many infectious agents and may produce a number of ECG abnormalities: Adams-Stokes syndrome, conduction disturbances, pseudoinfarction pattern, ST-segment and T-wave abnormalities, and premature ventricular contractions. Physicians should know the QTc interval in a patient to be treated with a quinolone or macrolide as these agents have proarrhythmic effects.
Lyme carditis is becoming a more frequent complication of Lyme disease, primarily due to the increasing incidence of this disease in the United States. Cardiovascular manifestations of Lyme disease often occur within 21 days of exposure and include fluctuating degrees of AV block, acute pericarditis or mild left ventricular dysfunction and rarely cardiomegaly or fatal pericarditis. AV block can vary from first-, second-, third-degree heart block, to junctional rhythm and asystolic pauses. Patients with suspected or known Lyme disease presenting with cardiac symptoms, or patients in an endemic area presenting with cardiac symptoms with no other cardiac risk factors should have a screening electrocardiogram along with Lyme titers. We present a case of third-degree AV block due to Lyme carditis, illustrating one of the cardiac complications of Lyme disease. This disease is usually self-limiting when treated appropriately with antibiotics, and does not require permanent cardiac pacing.
Adams- Stokes Syndrome The preferred name is cardiovascular syncope caused by heart block. It is marked by a sudden collapse into unconsciousness caused by a slow or absent pulse resulting in fainting with or without convulsions.
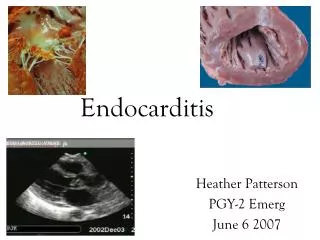
An inside View of Infective Endocarditis This cross-section shows vegetations (blood clots & bacteria) on the four heart valves.
Excised valve leaflets with large vegetation on ventricular side.
Prinzmetal’s angina, also known as variant angina, is a syndrome typically consisting of angina (cardiac chest pain) at rest that occurs in cycles. It is caused by vasospasm, a narrowing of the coronary arteries caused by contraction of the smooth muscle tissue in the vessel walls rather than directly by atherosclerosis (buildup of fatty plaque and hardening of the arteries). It was first described in 1959 by the American cardiologist Dr. Myron Prinzmetal (1908-1987).
Acute pericarditis classically shows widespread, concave-upward ST-segment elevation with PR-segment depression and PR-segment elevation in lead aVR. The ECG abnormalities may evolve through 4 phases: Stage I: diffuse ST-segment elevation and PR-segment depression (60-80% of cases); Stage II: normalization of the ST and PR segments, with flattening of the T wave; Stage III: widespread T-wave inversions; and Stage IV: normalization of the T waves. The prompt institution of therapy may prevent the appearance of all 4 stages.