Download
1 / 30
300 likes | 468 Views
Regional Mass Screening for Establishing the Prevalence of Alcohol Abuse in Pregnancy by Meconium Analysis. Joey Gareri HBSc. MSc. Candidate Motherisk Program, Hospital for Sick Children, Toronto Department of Pharmacology, University of Toronto, Toronto Grey Bruce Health Unit, Owen Sound

E N D
Regional Mass Screening for Establishing the Prevalence of Alcohol Abuse in Pregnancy by Meconium Analysis Joey Gareri HBSc. MSc. Candidate Motherisk Program, Hospital for Sick Children, Toronto Department of Pharmacology, University of Toronto, Toronto Grey Bruce Health Unit, Owen Sound Gideon Koren MD, FRCPC Hazel Lynn MD, MHSc.
BACKGROUND/RATIONALE biomarker development
FASD/FAS • Fetal Alcohol Spectrum Disorder (FASD) • A continuum of adverse fetal outcomes encompassing craniofacial dysmorphology, growth retardation, neurodevelopmental and cognitive deficits • Secondary Disabilities • “disrupted school experience” and “trouble with the law” • institutionalization/incarceration • unemployment/ dependent living • inappropriate or promiscuous sexual behaviour • mental health problems/substance addiction • Fetal Alcohol Syndrome (FAS) • Represents the far end of the “Spectrum” • Extreme phenotypic expression of heavy prenatal alcohol exposure
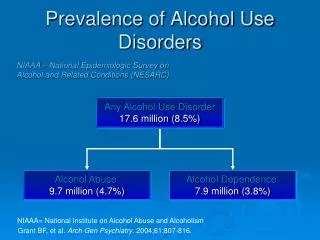
Public Health Impact In the general neonatal population… • ~1/100 are affected by Fetal Alcohol Spectrum Disorder • ~1/1000 are affected by Fetal Alcohol Syndrome Born to heavy-drinking mothers… • 4% of children have FAS • 40% of children have FASD
Diagnosis METHODS: 1) Cranio-facial features 2) Confirmation of in utero alcohol exposure -maternal self-reporting -maternal biomarkers of alcoholism *The use of any single or multiple maternal markers is not very effective in the identification of a drinking mother (Stoler et al., 1998) BIOMARKER SPECIFIC TO PREGNANCY
BACKGROUND/RATIONALE fatty acid ethyl esters (FAEE) as a biomarker
FAEE production Oxidative ACETALDEHYDE ADH and Microsomal Oxidation (e.g. CYP 2E1) FATTY ACYL CoA ETHANOL Acyl-coenzyme A:ethanol O-acyltransferase (AEAT) FAEE FATTY ACIDS FAEE Synthases POTENTIAL BIOLOGICAL MARKERS Non-Oxidative
Meconium as the Ideal Matrix • Meconium = baby’s first bowel movements (i.e. first few stools) • A matrix unique to the developing fetus that is already commonly used in neonatal drug screening • Superior to blood and urine • Discarded material • Collection is easy and non-invasive • Wide window of opportunity • Accumulation from 13th week gestation until birth
FAEE Meconium Analysis: Summary of Development • Ethanol metabolites produced by both mother and baby • Do not cross the placenta • FAEE in meconium are results of ONLY fetal metabolism of ethanol • Higher concentration of FAEE in neonates exposed to alcohol (Animal & Human Studies) • Baseline establishment (n=200) • Positive cut-off: 2.0 nmol total FAEE/g meconium • 100% Sensitive (0 false negatives) 98.4% Specific (low incidence of false positives)
FAEE Meconium Analysis: Implications of a Positive Result • 1st trimester exposure undetectable • Accidental exposure excluded • Social-drinkers fall below the baseline • Specific to heavy-drinking population • Positive result corresponds to sustained alcohol use through the latter two-thirds of pregnancy • Addiction-related use pattern
Grey Bruce, Ontario • Regional self-perception of excessive alcohol use • General alcohol use exceeds national average • CANADA: • 50% rate of regular alcohol use (Health Canada, 2002) • GREY BRUCE: • 74% rate of regular alcohol use (StatsCan, 2001) • Diverse populous • Urban centre (Owen Sound) • Rural/farming communities • Aboriginal communities • Amish communities • Proactive Public Health Unit
Making in-roads… • 1st population-based study using FAEE as a biomarker for heavy prenatal alcohol exposure • Co-operative collaboration between an urban-based research institution and regional health-care providers
Primary Hypothesis The fetal alcohol exposure rate as determined by FAEE analysis will exceed rates reported by epidemiological survey due to the lower sensitivity of maternal self-reporting.
Secondary Objectives • Reveal discernable expression patterns of the spectrum of FAEE that can be recovered from meconium (lauric, myristic, palmitic, palmitoleic, stearic, oleic, linoleic, linolenic, and arachidonic acid ethyl esters). • Assess the applicability of the FAEE meconium test as a population screening tool. • Increase public awareness of FAS and FASD in the region. • Increase awareness and diagnosis of FAS and FASD in the medical community of Grey-Bruce. • Create a model framework for future regional prevalence studies carried out in co-operation with public health departments and regional medical centres.
Study Design • Anonymous diaper collection • No supplemental information collected • maximal participation most accurate prevalence value • No Consent Required • Notification of “population health study supporting healthy child development” via posters on the wards • Assurance of anonymity • Right of refusal to provide a sample • Supplemental information (pamphlets) available upon request
Study Design • Duration: • January 1, 2004 – February 5, 2005 • 5 regional birthing centres + Grey-Simcoe midwives • Wiarton, Owen Sound, Markdale, Walkerton, Hanover • Regional Birth Rate: ~1,000 live births/year
Study Population • All neonates born in the five regional birthing centres • All neonates born via midwife (i.e. homebirth) in the region of Grey Bruce
METHODS:Sample Collection • Mom comes in for delivery • Nurse advises Mom about the study and provides her with a designated sealable bag • Baby is born • Mom or nurse changes soiled diaper • Mom/nurse places the diaper in the designated sealable bag • Nurse takes the bag and places it in a freezer • frozen diapers are collected periodically and the samples are analyzed
METHODS:FAEE Extraction/Analysis • Liquid-Liquid extraction (hexane:acetone) followed by Solid Phase extraction of FAEE from meconium (adapted by Chan et al.) • FAEE Analysis by Gas Chromatography • Confirmation of all positive and random negative samples via Mass Spectrometry
METHODS:FAEE Extraction/Analysis NEGATIVE POSITIVE
RESULTS:Sample Loss • LOST SAMPLES • 77 diapers non-sufficient quantity (<0.5 g) • ~70 diapers housekeeping error • 155 diapers not collected NO REPORTED REFUSALS Other Sources of Subject Loss • Patient diversion • extra-regional hospitals • Tertiary care: potentially important “high-risk” mothers
FAEE analysis 602 samples analyzed 26 positive results Fetal alcohol exposure rate: 4.32% Reported Alcohol Use in Pregnancy (U.S. statistics) Anonymous telephone survey(CDC 1997 & 2002) Prevalence of heavy drinking in pregnancy (>14 drinks/ week) is about 0.1% to 0.3% PRELIMINARY RESULTS:Prenatal Exposure Rate >14-fold higher than reported values
PRELIMINARY RESULTS:Positive vs. Negative Samples • Positive Samples (n = 26) • > 2 nmol/g • mean = 17.67 nmol/g • range • 2.23 - 144.18 nmol/g • Negative Samples (n = 576) • > LOQ (1 mg/mL)(n = 126) • mean = 0.46 nmol/g • range • 0.01 - 1.95 nmol/g
PRELIMINARY RESULTS:FAEE species distribution 2 short-chain esters not included in [FAEE] calculation Selective expression of longer-chain esters in positive samples
PRELIMINARY RESULTS:FASD awareness Public awareness • Public Health Rounds in Grey Bruce • March, 2004 Health-care awareness • Physician Grand Rounds • February, 2004 • GB Health Network administrators meeting • September, 2004
FUTURE WORK • GC-MS confirmation of positive results • Collection of further epidemiological data from regional authorities • comparison to “Parkin” intake questionnaire • Yes/No, drug/alcohol use in pregnancy • Analysis of remaining samples • Inclusion of St. Joseph’s Health Services in London, Ontario
Acknowledgements Canadian Institute for Health Research Hospital for Sick Children Dr. G. Koren MD Daphne Chan BSc Julia Klein MSc Dr. Bhushan Kapur PhD Chris Paciorek University of Toronto Dr. Cindy Woodland PhD Grey Bruce Public Health Unit Dr. Hazel Lynn Maureen Lapointe GBHS – Owen Sound Site Jeff Gonder Maryann Townsend GBHS – Wiarton GBHS – Markdale Site Val Marcella Suzie Furlong Hanover and District Hospital Vivian Nieson SGBHC – Walkerton Site Melody King Joanne McKee THANK YOU THE END