Download
1 / 28
290 likes | 467 Views
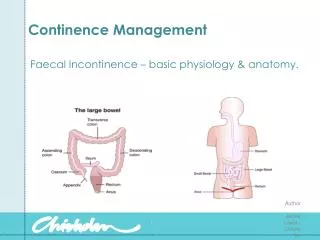
Continence Strategies: Towards Independence in the Elderly. Karina So Clinical Nurse Consultant Urology / Continence Management Concord Hospital. Practical strategies. Curative therapy for mild SI Symptom management for SI & UI Containment for severe and permanent Urinary incontinence

E N D
Continence Strategies: Towards Independence in the Elderly Karina So Clinical Nurse Consultant Urology / Continence Management Concord Hospital
Practical strategies • Curative therapy for mild SI • Symptom management for SI & UI • Containment for severe and permanent Urinary incontinence • Nocturnal incontinence • Risk management on IDC/SPC/CISC Urge incontinence is associated with a modest increase in falls. Chiarelli et. Al.(2008) Urinary incontinence is associated with an increase in falls: a systematic review” Australia Journal of Physiotherapy 55: 89-95
Stress incontinence (SI) Urge incontinence (UI) Mixed incontinence Overflow incontinence Functional incontinence Common Continence Problems in the elderly population
Stress Incontinence (SI) • Mild SI - Curative therapy • Pelvic Floor Muscle Exercises • Behavioural modification • Review medication(s) • Healthy diet & maintain healthy wt. • Regulate fluid intake & healthy bowel habit
Real-time Ultrasound Scan • Patientcan watch pelvic floor muscles contract and relax as you retrain them (visual feedback on performance). • It is a tool to encourage compliance. • It does not measure PFM strength.
Moderate SI Symptom management • Mild SI care path • Intravaginal device – pessary ring, tampon, Contiform device. • Selection of continence products uridome
Symptom management SI • Contiform! Penile clamp should be released every one to two hours to empty the bladder and prevent damage.
Severe and permanent SI Supportive care/ Risk Management • Containment • Social continence • Prevent skin problems, UTIs, odour control • Government Continence Aids schemes • PADP • CAAS/CAPS • DVA – gold card
Management of Urge Incontinence • Regulate fluid intake:amount,type, time. • Bladder training strategies +/- medication • Clothing- reduce layers, zipper/belt • Medications – dose, time, route. • Healthy diet, healthy bowel. • Selection of appropriate continence aids • Assess eligibility for Government schemes: PADP / CAAS/ DVA
Bladder Training therapy For mild-moderate sensory and motor urgency. • Deferment strategies (take control) • Pelvic floor muscle contractions • Talk to your bladder • Tactile sensation/pressure • Distraction (think hard) • Identify Optimal voiding time • Frequency, volume & urgency diary
Drugs used to treat OAB Anticholinergics/Antimuscurinic • Propantheline (Pro-banthine 15 - 30mg q.i.d.) • Oxybutynin (Ditropan 5mg up to q.i.d.) • Oxytrol transdermal patch (3.9mg twice a week) • Tolterodine (Detrusitol 1 - 2mg b.i.d.) • Darifenacin (Enablex) • Solifenacin (Vesicare 5 – 10mg daily)
Nocturnal incontinence Booster pad Pull up pants
Stricture therapy – patient specific • Identify the optimal time for urethral dilatation before a reduction in urine flow. • Select the size and type of firm catheter. • Educate and support patient to perform regular self dilatation. Coude tip firm nelaton catheter
Decompress the bladder using 100% silicone catheter size 14/16 Select the most appropriate drainage device – bag / valve Educate patient & carer on IDC care Management of Acute Urinary Retention
12 FG 14 FG 16 FG 18 FG 20 FG 22 FG 24 FG 3 ml 5 ml 10 ml 20 ml 30 ml 60 ml Catheter size Balloon Size Colour code
Management of Chronic Urinary Retention • Prevent recurrent symptomatic UTI • Identify high risk cases for urosepsis and prepare care plan • Use antibacterial soap for daily hygiene • If possible, high fluid intake > 2 litre/day • Prevent and correct constipation • Avoid trauma during catheter replacement procedure • Use catheter fixation device to avoid traction • Frequency of IDC or SPC replacement is individualised. • Periodic Urology review
Neurogenic bladder CISC +/- Anticholinergic Medication Queen Square Bladder Stimulator $75
Management of CISC • Reduce Symptomatic UTI – assess CISC technique, frequency of CISC, equipment care, single use versus reusable catheter. • Educate patient on monitoring of residual volume – bladder diary. • Periodic urology review.
Government Continence Aids Schemes • NSW Health – Enable Health • PADP • Federal Government Schemes • CAAS • CAPS from July 2010 • DVA for veterans with gold card
PADP Transition to Enable Health • Website: www.health.nsw.gov.au/health-public-affairs/factsheets • One centralised body • Office is based in Parramatta • Transfer of PADP data in stages
Continence Aids Assistance Scheme (CAAS) • CAAS is an Australian Government scheme offering assistance to eligible people who have permanent and severe incontinence. • The scheme covers children aged 5 to 15 years, and adults over 64 years with permanent incontinence due to neurological conditions (Cat.A). • The scheme also includes all causes of permanent incontinence, not just neurological causes, for those people who hold a pensioner concession card and their dependents (Cat.B). • Website: www.intouchdirect.com.au • The National Continence Helpline 1800 330 066
Continence Aids Payment Scheme (CAPS) As of July 2010 ….. • Clients can receive a one off payment of up to $489.95 to purchase their own products. • Can nominate the payment goes to an agency/ supplier. • CAPS payment is exempted as income. • Contact Medicare Australia Office for information 132 011
Role of Medicare Australia As of July 2010.. • Respond to enquires about CAPS. • Receive and process CAPS applications. • Make payments directly into a CAPS client’s nominated bank account or nominated provider’s account. • Send statements regarding the payment to clients. • Supply CAPS Application form