Download
1 / 19
190 likes | 313 Views
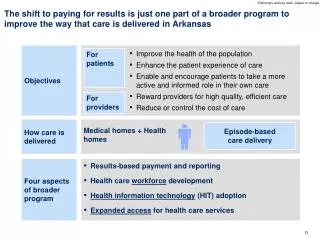
Lessons from Community-Based Initiatives to Expand Coverage and Improve Care Delivery Citizens’ Health Care Working Group May 12, 2005. Outline. Context for national funders’ investment Communities in Charge Findings Important Considerations Replicable Strategies & Strategies to Avoid.

E N D
Lessons from Community-Based Initiatives to Expand Coverage and Improve Care Delivery Citizens’ Health Care Working Group May 12, 2005
Outline • Context for national funders’ investment • Communities in Charge • Findings • Important Considerations • Replicable Strategies & Strategies to Avoid
Context Environment in which Programs were Conceived • Communities • Motivated • Issue of uninsured more tangible • Experiencing real financial pressures Federal/State Surpluses No Federal/State Solutions
Examples • Hillsborough County, FL • Milwaukee County, WI • Marian County, IN • Wayne County, MI
Raising the Question Robert Wood Johnson Foundation Communities in Charge W.K. Kellogg Foundation Community Voices Federal HRSA Community Access Program Could communities create and finance new coverage and delivery systems?
Objective Communities in Charge was a four year, $16.8M project of The Robert Wood Johnson Foundation to help communities design and implement new, or significantly expand existing, community-based systems for financing and delivering a full spectrum of care to the uninsured and under-insured
Expectations • Community-wide initiative • Result in systemic change • Serve a large number of uninsured individuals • Roughly modeled on Hillsborough HealthCare • Financing change to support new coverage • Restructuring of care delivery
Important Attributes • Large communities • Initial focus on coverage (versus access) • Emphasis on systematic process for design and implementation • Active coalitions (public-private partnerships) • Champions & Invested leaders • Plenty of providers
Funded Sites Spokane Portland Portland Buffalo Brooklyn AlamedaCo. D.C. San Mateo Co. Baltimore St. Louis Louisville Wichita Albuquerque Columbia Jackson Macon Austin Birmingham Jacksonville El Paso
3 Program Approaches • Public/Private Coverage (4) • Financing • Target populations • Public/Private Voluntary (4) • Other Public/Private (4)
Findings Location matters…because states differ • Medicaid eligibility thresholds • Medicaid disproportionate share distributions • Local responsibility for indigent medical care • “Riches”…and distributionof revenue
Findings Not every community has the “right stuff” • Key champions and invested senior leadership • Strong coalition with right people at the table • Keen knowledge of the fiscal and political commitments of critical partners • Awareness of local and state environment • Understanding of the community’s strengths and limitations • REAL resources
Findings Health care system is not a “system” for the uninsured • There are many gaps • There are many silos • Existing financing structures are a barrier to system change
Findings Communities can’t solve the coverage problem on their own • Without SIGNIFICANT state and/or federal financial assistance, community-based coverage programs cannot achieve the scale necessary to address need and ensure long-term sustainability
Findings Communities with the “right stuff” can impact how care for the uninsured is financed & delivered • Leveraging funds • Brokering public/private partnerships • Institutionalizing coalitions • Bridging gaps along the care continuum • Building and sustaining new safety net infrastructure • Facilitating outreach and enrollment in existing public programs
Important Considerations • Rethinking health care delivery and financing takes time, is hard work,requires $$$$, and is not for every community. • Big “P” and little “p” of politics as usual at local and state level can sink success of community efforts • Leadership is critical
Replicable Strategies • Health Policy Forums • Common eligibility screening tool • Shared clinical record • State/Federal partnership coverage programs • Coordinated gap-filling
Strategies to Avoid • ER “diversion” programs • Without significant incentives and outreach, will not change care seeking patterns • Real access to primary care and specialty services is required • Small business strategies • Well-documented challenges to overcoming the small business owner “cost” barrier • Examples
For More Information www.communitiesincharge.org http://www.statecoverage.net/pdf/issuebrief405.pdf Terry Stoller Program Director Communities in Charge Principal Medimetrix 1100 Republic Building 25 Prospect Avenue Cleveland, Ohio 44115 216-523-1300 x 3039 tstoller@mx.com