Download
1 / 38
591 likes | 2.37k Views
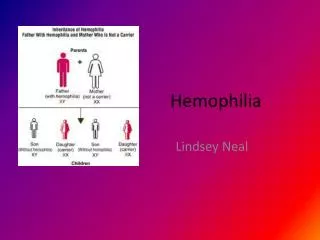
HEMOPHILIA. Inherited deficiency of factor VIII (hemophilia A) or factor IX (hemophilia B) Sex-linked inheritance; almost all patients male Female carriers may have mild symptoms Most bleeding into joints, muscles; mucosal and CNS bleeding uncommon

E N D
HEMOPHILIA • Inherited deficiency of factor VIII (hemophilia A) or factor IX (hemophilia B) • Sex-linked inheritance; almost all patients male • Female carriers may have mild symptoms • Most bleeding into joints, muscles; mucosal and CNS bleeding uncommon • Severity inversely proportional to factor level < 1%: severe, bleeding after minimal injury 1-5%: moderate, bleeding after mild injury > 5%: mild, bleeding after significant trauma or surgery
GENETICS OF HEMOPHILIA • About half of cases of hemophilia A due to an inversion mutation in intron 1 or 22 • Remainder genetically heterogeneous • Nonsense/stop mutations prevent factor production • Missense mutations may affect factor activity rather than production • 15-20% of cases due to new mutations
Deficiency of factor VIII or IX affects the propagation phase of coagulation • Most likely to cause bleeding in situations where tissue factor exposure is relatively low
ACUTE COMPLICATIONS OF HEMOPHILIA Hemarthrosis (joint bleeding) Muscle hematoma (pseudotumor)
Joint destruction Nerve damage LONG-TERM COMPLICATIONS OF HEMOPHILIA
Hemophilic arthropathy “Target joint” = irreversibly damaged joint with vicious cycle of injury and repeated bleeding
Hemophilic arthropathy J Thromb Hemost 2010;8:1895
Hemophilic arthropathyVariable relationship between # of joint bleeds and severity Green line: Evidence of early joint damage with relatively few bleeds Yellow line: Linear relationship between # of bleeds and joint damage Red line: Joint damage occurs after threshold # bleeds Blue line: Little joint damage despite many bleeds J Thromb Hemost 2010;8:1895
Management of hemophilic arthropathy • Physical therapy • Weight control • COX-2 inhibitors safe and effective • Judicious use of opioids • Surgical or radionuclide synovectomy • Joint replacement
OTHER COMPLICATIONS OF HEMOPHILIA • Pseudotumor: gradually enlarging cyst in soft tissue or bone (requires surgery) • Retroperitoneal hemorrhage • Bowel wall hematoma • Hematuria → renal colic (rule out structural lesion) • Intracranial or intraspinal bleeding (rare but deadly) – usually after trauma
HEMOPHILIATreatment of bleeding episodes • Unexplained pain in a hemophilia should be considered due to bleeding unless proven otherwise • External signs of bleeding may be absent • Treatment: factor replacement, pain control, rest or immobilize joint • Test for inhibitor if unexpectedly low response to factor replacement
Dosing clotting factor concentrate • 1 U/kg of factor VIII should increase plasma level by about 2% (vs 1% for factor IX) • Half-life of factor VIII 8-12 hours, factor IX 18-24 hours • Volume of distribution of factor IX about twice as high as for factor VIII • Steady state dosing about the same for both factors – initial dose of factor IX should be higher
Give factor q 12 hours for 2-3 days after major surgery, continue with daily infusions for 7-10 days • Trough factor levels with q 12 h dosing after major surgery should be at least 50-75% • Most joint and muscle bleeds can be treated with “minor” (50%) doses for 1-3 days without monitoring
FACTOR VIII CONCENTRATE • Recombinant • Virus-free, most expensive replacement • Treatment of choice for younger/newly diagnosed hemophiliacs • Somewhat lower plasma recovery than with plasma-derived concentrate • Highly purified • Solvent/detergent treated, no reports of HIV or hepatitis transmission • Intermediate purity (Humate-P™) • Contains both factor VIII and von Willebrand factor • Solvent/detergent treated, no reports of HIV or hepatitis transmission • Mainly used to treat von Willebrand disease
FACTOR IX CONCENTRATE • Recombinant (slightly lower plasma recovery) • Highly purified (solvent/detergent treated, no reports of virus transmission) • Prothrombin complex concentrate • Mixture of IX, X, II, VII • Low risk of virus transmission • Some risk of thrombosis
DDAVP • Releases vWF/fVIII from endothelial cells • Factor VIII levels typically rise 2-4 fold after 30-60 min (IV form) or 60-90 min (intranasal) • Enhanced platelet adhesion due to ↑ vWF • Useful for mild hemophilia (VIII activity > 5%) prior to dental work, minor surgery etc • Trial dose needed to ensure adequate response • Cardiovascular complications possible in older patients
Bethesda Assay for Inhibitors • Serial dilutions of patient plasma in normal plasma • Incubate 2 hours • Assay residual factor activity • 1 Bethesda Unit neutralizes 50% of factor in an equivalent volume of normal plasma • Example: 1:100 dilution of patient plasma + normal plasma → 50% residual factor activity, so inhibitor titer is 100 BU
Bethesda Assay 50% Residual factor activity 100 BU 1:1 1:10 1:100 1:1000 dilution pt plasma
TREATMENT OF HEMOPHILIACS WITH INHIBITORS • Recombinant factor VIIa • FEIBA (Factor Eight Inhibitor Bypassing Activity) • Mixture of partially activated vitamin K-dependent clotting proteases including VIIa • High dose factor VIII (if low titer inhibitor) • Induction of tolerance with daily factor VIII infusions • Optimal dose not established • Role for concomitant immunosuppression?
Liver disease in hemophilia • Hepatitis C still a problem, though incidence falling with safer factor concentrates • Treatment for hepatitis C with interferon often causes thrombocytopenia • Liver transplantation done occasionally (cures hemophilia) • All newly diagnosed hemophiliacs should be vaccinated against hepatitis A and B
ACQUIRED FACTOR VIII DEFICIENCY • Due to antibody to factor VIII (most common autoimmune factor deficiency) • Most patients elderly • Often presents with severe soft tissue or mucosal bleeding (different bleeding pattern than inherited hemophilia) • Laboratory: prolonged aPTT not corrected by mixing, very low factor VIII activity • Normal INR, thrombin time and platelet count • Treatment: rVIIa, FEIBA, immunosuppression
VON WILLEBRAND DISEASE • Common (most common?) inherited bleeding disorder • Partial lack of VWF causes mild or moderate bleeding tendency • Menorrhagia, bleeding after surgery, bruising • Typically autosomal dominant with variable penetrance • Laboratory: • Defective platelet adherence (PFA-100) or long bleeding time • Subnormal levels of von Willebrand antigen and factor VIII in plasma • Low Ristocetin cofactor activity or VWF activity
VON WILLEBRAND DISEASE • Type 1 – decreased production of vWF • Levels 20-50%, antigen ≈ activity • Type 2 – qualitative defect (missense mutation) • Several different types • Usually a disproportionate decrease in vWF activity vs antigen • Type 3 – severe deficiency • Antigen, activity and factor VIII levels < 10% • Hemophilia-like phenotype • Recessively inherited
Type 2 vWD • 2A: Selective deficiency of large multimers • Defective assembly • Increased susceptibility to proteolysis • 2B: Increased affinity for platelet Gp Ib • Large multimers bind spontaneously to platelets and cleared from blood • Rarely, a mutation in Gp Ib may have the same effect (“platelet-type” vWD) • 2M: Decreased vWF function but no loss of large multimers • 2N: Decreased binding of factor VIII to vWF (recessive)
Weibel-Palade body (arrows) in the cytoplasm of endothelial cell. N - nucleus. Scale = 100 nm. (Human, skin.)
Desmopressin (DDAVP) in vWD • DDAVP releases vWF from endothelial cells • Can be given IV or intranasally • 0.3 mcg/kg IV, or 150 mcg per nostril • Typically causes 2-4 fold increase in blood levels of vWF (in type 1 vWD), with half-life of 8+ hours • Response to DDAVP varies considerably • Administration of a trial dose necessary to ensure a given patient responds adequately • Peak response • Duration of response
Indications for clotting factor concentrate administration in vWD • Type 2 or 3 vWD • Active bleeding • Surgery or other invasive procedure • Type 1 vWD with inadequate response to DDAVP
Acquired von Willebrand disease • Monoclonal gammopathy: vWF neutralized by paraprotein (?) • Autoimmune disorders: Autoantibody to vWF • Myeloproliferative disorder: large multimers absorbed onto neoplastic cells (platelets?) • Cardiovascular diseases (AS, VSD, etc): High shear stress causes unfolding/proteolysis of large multimers • Hypothyroidism: Decreased release of vWF from endothelial cells • Treatment varies depending on cause/mechanism
ACQUIRED VON WILLEBRAND DISEASE NEJM 2009;361:1887