Download
1 / 1
10 likes | 142 Views
Genetic disease involving the Human alpha glucosidase gene Stephen Perritt, Ben Ernest, and Elizabeth Johnson UTK and GST Funded by NIH, ISMD Award # 1R25GM086761-01. Mutations. Pompe’s Disease. At present more than 200 different mutations in the acid α-glucosidase gene are known.

E N D
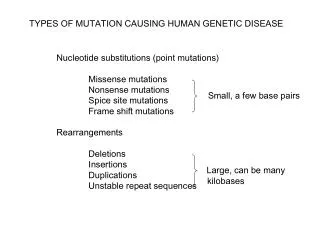
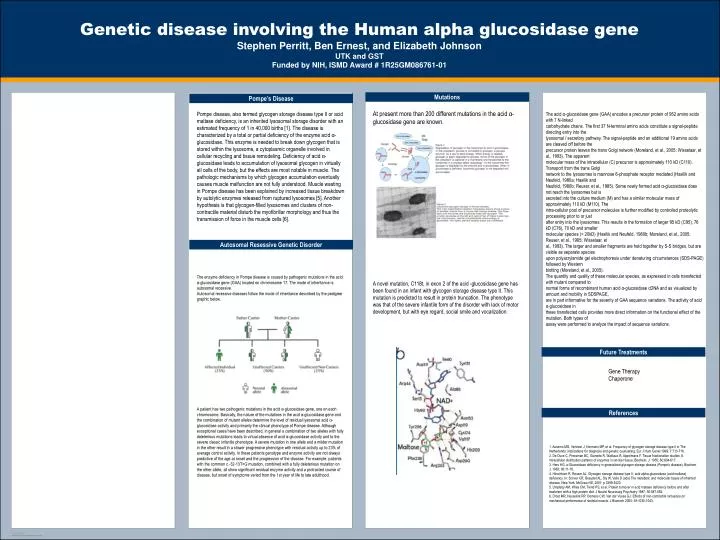
Genetic disease involving the Human alpha glucosidase gene Stephen Perritt, Ben Ernest, and Elizabeth JohnsonUTK and GST Funded by NIH, ISMD Award # 1R25GM086761-01 Mutations Pompe’s Disease At present more than 200 different mutations in the acid α-glucosidase gene are known. Pompe disease, also termed glycogen storage disease type II or acid maltase deficiency, is an inherited lysosomal storage disorder with an estimated frequency of 1 in 40,000 births [1]. The disease is characterized by a total or partial deficiency of the enzyme acid α-glucosidase. This enzyme is needed to break down glycogen that is stored within the lysosome, a cytoplasmic organelle involved in cellular recycling and tissue remodeling. Deficiency of acid α-glucosidase leads to accumulation of lysosomal glycogen in virtually all cells of the body, but the effects are most notable in muscle. The pathologic mechanisms by which glycogen accumulation eventually causes muscle malfunction are not fully understood. Muscle wasting in Pompe disease has been explained by increased tissue breakdown by autolytic enzymes released from ruptured lysosomes [5]. Another hypothesis is that glycogen-filled lysosomes and clusters of non-contractile material disturb the myofibrillar morphology and thus the transmission of force in the muscle cells [6]. The acid α-glucosidase gene (GAA) encodes a precursor protein of 952 amino acids with 7 N-linked carbohydrate chains. The first 37 N-terminal amino acids constitute a signal-peptide directing entry into the lysosomal / secretory pathway. The signal-peptide and an additional 19 amino acids are cleaved off before the precursor protein leaves the trans Golgi network (Moreland, et al., 2005; Wisselaar, et al., 1993). The apparent molecular mass of the intracellular (C) precursor is approximately 110 kD (C110). Transport from the trans Golgi network to the lysosomes is mannose 6-phosphate receptor mediated (Hasilik and Neufeld, 1980a; Hasilik and Neufeld, 1980b; Reuser, et al., 1985). Some newly formed acid α-glucosidase does not reach the lysosomes but is secreted into the culture medium (M) and has a similar molecular mass of approximately 110 kD (M110). The intra-cellular pool of precursor molecules is further modified by controlled proteolytic processing prior to or just after entry into the lysosomes. This results in the formation of larger 95 kD (C95), 76 kD (C76), 70 kD and smaller molecular species (< 20kD) (Hasilik and Neufeld, 1980b; Moreland, et al., 2005; Reuser, et al., 1985; Wisselaar, et al., 1993). The larger and smaller fragments are held together by S-S bridges, but are visible as separate species upon polyacrylamide gel electrophoresis under denaturing circumstances (SDS-PAGE) followed by Western blotting (Moreland, et al., 2005). The quantity and quality of these molecular species, as expressed in cells transfected with mutant compared to normal forms of recombinant human acid α-glucosidase cDNA and as visualized by amount and mobility in SDSPAGE, are in part informative for the severity of GAA sequence variations. The activity of acid α-glucosidase in these transfected cells provides more direct information on the functional effect of the mutation. Both types of assay were performed to analyze the impact of sequence variations. A novel mutation, C118t, in exon 2 of the acid -glucosidase gene has been found in an infant with glycogen storage disease type II. This mutation is predicted to result in protein truncation. The phenotype was that of the severe infantile form of the disorder with lack of motor development, but with eye regard, social smile and vocalization. Autosomal Resessive Genetic Disorder The enzyme deficiency in Pompe disease is caused by pathogenic mutations in the acid α-glucosidase gene (GAA) located on chromosome 17. The mode of inheritance is autosomal recessive. Autosomal recessive diseases follow the mode of inheritance described by the pedigree graphic below. A patient has two pathogenic mutations in the acid α-glucosidase gene, one on each chromosome. Basically, the nature of the mutations in the acid α-glucosidase gene and the combination of mutant alleles determine the level of residual lysosomal acid α-glucosidase activity and primarily the clinical phenotype of Pompe disease. Although exceptional cases have been described, in general a combination of two alleles with fully deleterious mutations leads to virtual absence of acid α-glucosidase activity and to the severe classic infantile phenotype. A severe mutation in one allele and a milder mutation in the other result in a slower progressive phenotype with residual activity up to 23% of average control activity. In these patients genotype and enzyme activity are not always predictive of the age at onset and the progression of the disease. For example, patients with the common c.-32-13T>G mutation, combined with a fully deleterious mutation on the other allele, all show significant residual enzyme activity and a protracted course of disease, but onset of symptoms varied from the 1st year of life to late adulthood. Future Treatments Gene Therapy Chaperone References 1. Ausems MG, Verbiest J, Hermans MP, et al. Frequency of glycogen storage disease type II in The Netherlands: implications for diagnosis and genetic counselling. Eur J Hum Genet 1999; 7:713-716. 2. De Duve C, Pressman BC, Gianetto R, Wattiaux R, Appelmans F. Tissue fractionation studies. 6. Intracellular distribution patterns of enzymes in rat-liver tissue. Biochem. J. 1955; 60:604-617. 3. Hers HG. a-Glucosidase deficiency in generalized glycogen storage disease (Pompe's disease). Biochem. J. 1963; 86:11-16. 4. Hirschhorn R, Reuser AJ. Glycogen storage disease type II; acid alpha-glucosidase (acid maltase) deficiency. In: Scriver CR, Beaudet AL, Sly W, Valle D (eds) The metabolic and molecular bases of inherited disease. New York: McGraw-Hill, 2001: p 3389-3420. 5. Umpleby AM, Wiles CM, Trend PS, et al. Protein turnover in acid maltase deficiency before and after treatment with a high protein diet. J Neurol Neurosurg Psychiatry 1987; 50:587-592. 6. Drost MR, Hesselink RP, Oomens CW, Van der Vusse GJ. Effects of non-contractile inclusions on mechanical performance of skeletal muscle. J Biomech 2005; 38:1035-1043.