Download
1 / 31
380 likes | 820 Views
Evaluation of Thyroid Nodules. Eric Oliver August 30, 2007. Objectives. Discuss Common Causes of Thyroid Nodules Highlight Application of Imaging Studies in Evaluation of the Thyroid Nodule. The Thyroid Nodule.

E N D
Evaluation of Thyroid Nodules Eric Oliver August 30, 2007
Objectives • Discuss Common Causes of Thyroid Nodules • Highlight Application of Imaging Studies in Evaluation of the Thyroid Nodule
The Thyroid Nodule • It is estimated that the prevalence of thyroid nodules in the general population is 4 - 7%. • Benign adenomas or cysts account for approximately 90% of detected thyroid nodules. • In the U.S., ~10,000 to 17,000 new cases of primary thyroid cancer are diagnosed each year. • 1,000 - 2,000 people die each year from primary thyroid carcinomas.
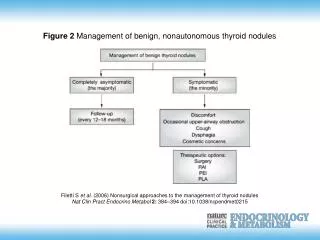
Causes of Thyroid Nodularity • Benign • Follicular Adenomas • Multinodular goiter (colloid adenoma) • Hashimoto’s thyroiditis • Cysts (colloid, simple, hemorrhagic)
Causes of Thyroid Nodularity • Malignant • Papillary Carcinoma • Follicular Carcinoma • Medullary Carcinoma • Anaplastic and poorly differentiated carcinoma • Primary lymphoma of the thyroid • Metastatic carcinoma (especially breast and renal cell carcinoma)
Low Suspicion • Family history of autoimmune disease (eg, Hashimoto’s thyroiditis) • Family history of benign thyroid nodule or goiter • Presence of thyroid hormonal dysfunction • Pain or tenderness associated with nodule • Soft, smooth, and mobile nodule
Hegedus: N Engl J Med, Volume 351(17).October 21, 2004.1764-1771
Case 1 A 16 year old female is seen because of a 6 month history of fatigue, nervousness, tremor, heat intolerance, polyphagia and weight loss. Her scholastic work has declined in quality. Recently she noticed some enlargement of her neck and prominence of her eyes. Physical examination reveals: B.P. 130/60 mm Hg., pulse 96/minute, smooth warm skin, eyelid retraction, symmetric thyroid enlargement, fine hand tremor and mild muscle weakness. Her TSH is low.
Low TSH • Suspect independently functioning thyroid • ~10 percent of patients with a solitary nodule have a suppressed level of serum thyrotropin • Next Step: Scintography
Radionuclide Scanning • Used to identify whether a nodule is functioning. • Functioning nodules are nearly always benign • Approximately 90 percent of nodules are nonfunctioning • 5 percent of nonfunctioning nodules are malignant • Thus, in the patient with a suppressed level of serum thyrotropin, radionuclide confirmation of a functioning nodule may obviate the need for biopsy.
Scintigraphy • Usually either Technetium or Radioiodine • Normal follicular cells will trap both but only radioiodine is added to tyrosine and stored in the colloid space • Both benign and almost all malignant neoplastic tissue concentrate both radioisotopes less than normal thyroid tissue • 5-8% of warm or cold nodules are malignant
Cold Nodules • Thyroiditis • Fibrosis • Cyst • Non-functioning Adenoma • Multinodular Goiter • Malignancy
Hot Nodules • Functioning Adenoma • Thyroiditis • Multinodular goiter
Limitations of Scintigraphy • Two dimensional scanning technique • Inability to measure the size of a nodule accurately • Missed malignant thyroid nodules
Case 2 TR is a 40 year old female who presents for her annual physical. On exam, you palpate a 1.5x 2 cm nodule in the right lobe of her thyroid gland. The nodule is non-tender and mobile. Both her TSH and free T4 are normal. What test would you order next?
Ultrasonography • Facilitate fine needle aspiration biopsy of a nodule • Assess the comparative size of nodules, lymph nodes, or goiters in patients who are under observation or therapy • Evaluate for recurrence of a thyroid mass after surgery
Fine-Needle Aspiration Biopsy • Most important step in the diagnostic evaluation of thyroid nodules, exception would include hyperthyroidism where scintigraphy should be performed first or highly suspicious exams warranting immediate surgery. • Mean sensitivity higher than 80% and specificity higher than 90%. • Can categorize tissue into the following diagnostic categories: malignant, benign, thyroiditis, follicular neoplasm, suspicious, or nondiagnostic • Cost Effective – some studies estimate that it reduces cost by 25 % and reduce the need for diagnostic thyroidectomy by 20-50%.
FNAB Limitations • Hypocellular aspirates may be observed in cystic nodules, or they may be related to biopsy technique. • The absence of malignant cells in an acellular or hypocellular specimen does not exclude malignancy. • Inability to reliably distinguish a benign follicular neoplasm from a malignant neoplasm. • Aspirates may be required from multiple sites of the nodule to improve sampling.
Case 3 • F.H. is a 66 year old man who complains of a “a bump in his throat.” He states that he has also developed some discomfort while eating more recently. PMH is significant for childhood neck irradiation. There is no palpable mass on exam and oropharynx is clear.
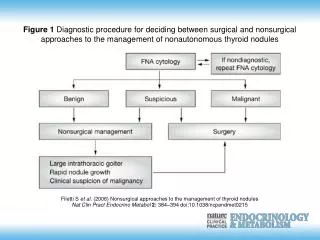
Algorithm for the Cost-Effective Evaluation and Treatment of a Clinically Detectable Solitary Thyroid Nodule Hegedus: N Engl J Med, Volume 351(17). October 21, 2004. 1764-1771
Take Home Points • Hyperfunctioning nodules (Low TSH, High T3/T4) are almost always benign and biopsy is generally not recommended. Scintigraphy may aid in evaluation and treatment. • Consider FNAB for patients with normal and hypofunctioning nodules. • Patients in which there is a high suspicion can immediately be referred to ENT for surgery.
References • http://www.thyroidmanager.org/FunctionTests/ultra-frame.htm • Ford. Evaluation of Thyroid Nodules. http://ctm.stanford.edu/06-07/Thyroid%20Nodule_Ford_6_18_07.pdf • Hegedus: N Engl J Med, Volume 351(17).October 21, 2004.1764-1771 • Miller. Management of Thyroid Nodules. Radiology Rounds. MGH Department of Radiology. 2005. http://www.massgeneralimaging.org/newsletter/march_2005 • Nguyen GK. Fine-needle aspiration of the thyroid: an overview. CytoJournal 2005, 2:12 http://bmc.ub.uni-potsdam.de/1742-6413-2-12/ • Ross. Evaluation of the Thyroid Nodule. J Nucl Med 1991; 32:2181-2192. • Society of Nuclear Medicine Procedure Guideline for Thyroid Scintigraphy. 1999. http://interactive.snm.org/docs/pg_ch05_0403.pdf