Download
1 / 22
320 likes | 632 Views
An interesting case of Median Arcuate Ligament Syndrome. BSGAR submission 6-8 th February 2019 Coomer W, Jeffries J, Pallas R, Parry C, Eynon A, Foliaki A, Ellis-Owen R. Objectives. Clinical information Figures Final Diagnosis Key learning points Discussion. Clinical information.

E N D
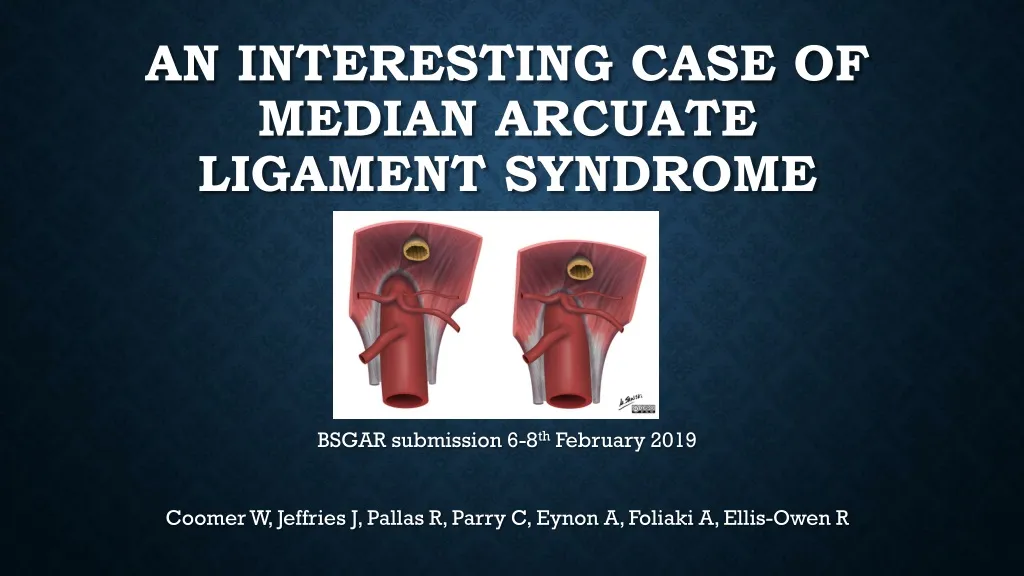
An interesting case of Median Arcuate Ligament Syndrome BSGAR submission 6-8th February 2019 Coomer W, Jeffries J, Pallas R, Parry C, Eynon A, Foliaki A, Ellis-Owen R
Objectives Clinical information Figures Final Diagnosis Key learning points Discussion
Clinical information HPC • 20F student • Presented with 2 day history of severe post-prandial abdominal pain and vomiting. • Mild weight loss • FBC - Hb 137, WCC 7.3, Plts 262 • U/E normal. CRP 1 PMH • Cholecystectomy, Appendicectomy, Ehler’sDahnlos syndrome • Previous coeliac artery stenosis diagnosed in USA 1 year previously • This required PICC line insertion and TPN feeding CT scan requested by surgical on call team…
Median arcuate ligament Ligament formed at the base of the diaphragm Unites the left and right diaphragmatic crura near T12 vertebra Fibrous arch forms anterior aspect of the aortic hiatus - through which the aorta, thoracic duct and azygous vein pass
Median arcuate ligament syndrome Vague constellation of symptoms which can include : • epigastric pain, postprandial pain, chronic non-specific abdominal pain, nausea, vomiting, weight loss Often a diagnosis of exclusion – reliant on clinical features and imaging findings Investigations include – CT angiogram and duplex ultrasonography CT – focal narrowing of coeliac artery with post-stenotic dilatation USS – Peak systolic velocities of >200cm/s are suggestive of MALS
Management of MALS Controversial! Kim et al (2016) performed meta-analysis of accurate diagnosis and successful treatment for patients with MALS • Imaging techniques included : Mesenteric duplex ultrasonography, CT angiography, MR angiography, gastric tonometry, and mesenteric arteriography • Surgical interventions included : open, laparoscopic, or robotic ligament release; celiac ganglionectomy; and coeliac artery revascularization You et al (2013) compared open laparotomy vs robotic assisted laparoscopic approach – complete resolution of symptoms 1 month post-operatively Angioplasty with stenting has been used in recalcitrant cases
Final diagnosis in our case study Diagnosis of MALS made Patient under care of Upper GI surgeon and decision made for theatre Laparoscopic release of Median Arcuate Ligament performed OUTCOME • Patient’s post-prandial pain improved following surgery • continued to suffer with nausea and vomiting • Post surgical contrast swallow showed no mechanical cause for vomiting
Key learning points • Importance of understanding past medical history when interpreting scan • MALS often a diagnosis of exclusion – consider other investigations primarily • Awareness of median arcuate ligament syndrome as possibility for coeliac axis stenosis • Treatment options – including conservative, surgical, ??interventional
discussion This case highlights complexity of diagnosis of MALS Diagnostic workup and therapeutic intervention can be challenging Why the symptoms? Several theories • Compression of coeliac axis causes ischaemia, or decreased blood flow to abdominal organs – causing abdominal pain. • Ligament causes compression of coeliac ganglia which can lead to pain Keep MALS in mind with patients with symptoms that may include post-prandial pain, chronic mesenteric pain, weight loss
References Case courtesy of Dr Matt Skalski, Radiopaedia.org, rID: 36837 ‘Median Arcuate Ligament Syndrome—Review of This Rare Disease’.Kim et al, JAMA surg, 2016;151(5):471-477. doi:10.1001/jamasurg.2016.0002 ‘Treatment of Median Arcuate Ligament Syndrome Via Traditional and Robotic Techniques’ . You et al, Hawaii Journal of Medical Public Health. 2013 Aug; 72(8): 279–281