Download
1 / 47
490 likes | 947 Views
Elder Abuse. Dr. Edward Warren Chair, Geriatrics Carolinas Campus June 2012. GOALS. Define elder abuse and its types. Explain the role of Adult Protective Services. Discuss the concept of mandated reporter. Screen for elder abuse . Order proper testing for elder abuse.

E N D
Elder Abuse Dr. Edward Warren Chair, Geriatrics Carolinas Campus June 2012
GOALS • Define elder abuse and its types. • Explain the role of Adult Protective Services. • Discuss the concept of mandated reporter. • Screen for elder abuse. • Order proper testing for elder abuse. • Report elder abuse competently and document it properly.
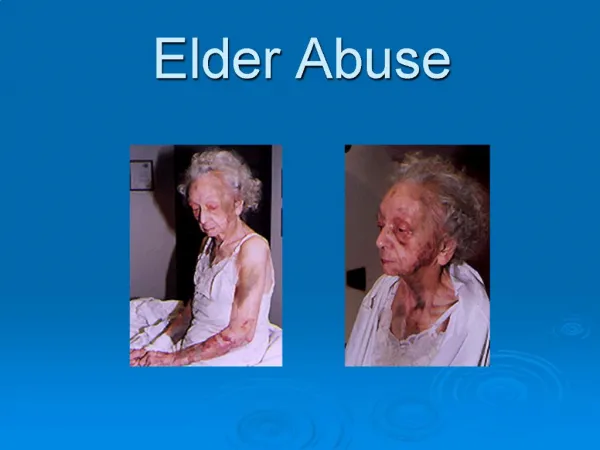
Definition of Elder Abuse Elder abuse is doing something or failing to do something that results in harm to an elderly person or puts a helpless older person at risk of harm. This includes • Physical, sexual, and emotional abuse • Neglecting or deserting an older person for whom you are responsible • Taking or misusing an elderly person's money or property
Elder Abuse? • Elder abuse happens within the family. • It happens in hospitals, nursing homes, and in the community. • Elder abuse is a serious problem in this country. All 50 states have laws against elder abuse. The laws differ, but all states have systems for reporting suspected abuse. • http://www.nlm.nih.gov/medlineplus/elderabuse.html
EPIDEMIOLOGY • Every year an estimated 2.1 million older Americans are victims of physical, psychological, or other forms of abuse and neglect. • Factors such as fear, shame, guilt, or ignorance play a role in the underestimation of elder abuse. • Studies routinely exclude those unable to respond to a survey, non-English speakers, and persons with mental illness, further limiting the accuracy of the count.
AdultProtectiveServices (APS) is a program of most states that looks out for abused adults among other things.The APS program is state supervised and locally administered through local, county, departments of social services. Adult Protective Services
APS Service Population Services are provided to: • adults age 60 and over and • incapacitated persons ages 18 to 59 who have been abused, neglected or exploited, or are at risk of abuse, neglect, or exploitation, without regard to income or resources.
Incapacitation • An adult who is impaired by: - mental illness - mental retardation - physical illness or disability - advanced age - other causes • to the extent that the adult lacks sufficient understanding or capacity to make, communicate or carry out reasonable decisions regarding his/her well being.
Rights of Adults Competent adults have the right to refuse services even if everyone involved in the case believes that assistance is needed.
FY 2007 APS Statistics In FY 2007, 13,515 reports of adult abuse, neglect, and/or exploitation were received by local departments of social services in Virginia. 65% of APS reports were substantiated.
Who Are the Victims? • Elder abuse occurs among members of all racial, socioeconomic, and religious backgrounds. • FY 2007 APS Reports in Virginia - 68% over age 60 - 32% ages 18–59 and incapacitated - 63% women - 37% men - 72% white - 24% African-American
Living Arrangements of Subject at Time of Report • 62% own home or apt • 13% other’s home or apt • 10% nursing facilities • 7% assisted living facilities • 4% DMHMRSAS facilities • (Dept of Mental Health, Mental Retardation and Substance Abuse Services) • 2% other setting • 2% shelter or are homeless
Typical Victim Typical victim: • White • Widowed • Female • Mid 70’s or older • Limited income • Usually lives with the perpetrator, who is often the spouse or adult child.
Reporter in FY 2007 in Virginia? • Family/Relative – 35% • Physician –8%* • Friend/Neighbor –6% • Social Worker –6%* • Self – 5% • ALF & Nursing Home Staff—6%* • Nurse –3%* • Law enforcement – 3%* • VDSS Staff (inc. Licensing Programs staff) – 1%* • Financial institution – <1% * Mandated reporters
Challenges -Illness, frailty or dementia may mask abuse or neglect. - Social isolation increases risk and difficulty of identifying mistreatment. • Stereotypes about aging and disability. • Reluctance to interfere or get involved in a family matter, especially financial exploitation.
Types of Elder Abuse • Physical abuse of the elderly • Emotional abuse of the elderly (psychological or verbal) • Neglect or abandonment of elders by caregivers • Self-neglect by elders • Sexual abuse of the elderly • Financial exploitation of seniors (elder financial abuse) • Healthcare fraud or healthcare abuse of the elderly
What is Physical or Verbal Abuse? Willful infliction of physical pain, injury or mental anguish or unreasonable confinement. • Wounding, scratching, bruising, burning • Verbal assaults, threats, intimidation • Broken bones, sprains, dislocations • Shoving, beating, kicking adult • Restrained, tied to bed or chair, locked in
What is Sexual Abuse? An act committed with the intent to sexually molest, arouse or gratify any person • Intentional touching intimate parts or material covering them • Forcing the adult to touch the adult’s own or another's intimate parts or material covering them • Forcing another person to touch the adult’s intimate parts or material covering them
What is Neglect & Self-Neglect? Living under such circumstances that the adult is not able to provide, or is not provided, services to maintain physical and mental health and well-being • Malnourished • Soiled bedding, furniture or clothing • Unsafe or hazardous living conditions • Lacking needed medication • Lacking heat, running water, or electricity
What is Exploitation? Illegal use of the adult’s resources for another’s profit or advantage • Missing personal belongings • Changed will or POA • Large bank withdrawals • Unpaid bills • Excessive payment for care or services • Documents contain suspicious signatures • Sudden appearance of previously uninvolved relatives or friends
Abuse Perpetrators Can Be: • Families Members • Paid Caregivers • Friends • Facility Staff Members • Agency Staff Members • Handy Men/Contractors • Con Artists
Causative Theories Theories of the origin of mistreatment of elders have been divided into 4 major categories, as follows: • physical and mental impairment of the patient • caregiver stress • transgenerational violence • psychopathology in the abuser.
History: • The American Medical Association recommends that doctors routinely ask geriatric patients about abuse, even if signs are absent. • Keep questions direct and simple • Ask in a nonjudgmental or non-threatening manner to increase the likelihood of a candid response. • Interview the patient and the caregiver separately • To detect disparities offering clues to the diagnosis of abuse • Document carefully!
History: • Physical abuse • Are you afraid of anyone at home? • Have you been struck, slapped, or kicked? • Have you been tied down or locked in a room? • Have you been force-fed? • Psychological abuse • Do you ever feel alone? • Have you been threatened with punishment, deprivation, or institutionalization? • Have you received "the silent treatment"? • What happens when you and your caregiver disagree?
History: • Sexual abuse: • Has anyone touched you in a sexual way without permission? • Neglect • Do you lack items such as eyeglasses, hearing aids, or false teeth? • Have you been left alone for long periods? • Is your home safe? • Do you get help when it is needed? • Financial abuse • Is money being stolen from you or used inappropriately? • Have you been forced to sign a power of attorney, will, or another document against your wishes? • Have you been forced to make purchases against your wishes? • Does your caregiver depend on you for financial support?
History: • Follow-up questions (if abuse is identified) • How long has the abuse been occurring? • Is it an isolated incident? • Why do you think this happens? • When do you think the next episode will occur? • Is the abuser present here? • Is it safe for you to return home? • What would you like to see happen? • Have you ever received help for this problem before?
Documentation • Accurate and thorough documentation of the history and physical examination in cases of suspected elder abuse is essential. • The history of any suspected types of abuse, as well as the mechanism of injury, should be documented in the patient‘s own words, if possible.
Documentation Documentation should include: • Details of the pertinent social history (e.g., caregiver‘s identity, living arrangements, functional status). • A description of any injuries should include types of injuries (e.g., fractures, lacerations, contusions), number, size, location, color, and stage of healing or approximate ages of the injuries.
Documentation Documentation should include: • Photographs of the injuries should be taken before treatment. In the absence of photographs, the locations and types of injuries should be documented on a body map or diagram. • The explanation given by the patient for the mechanism of each injury, as well as comments about whether the explanation seems appropriate.
Documentation • Laboratory investigations and imaging studies • Follow-up plans, referrals, and interventions • In cases of suspected elder abuse that result in legal action, thorough documentation may be critical in determining the outcome and ultimate care of the patient.
Observations that Raise Suspicion • Several injuries in various stages of evolution • Unexplained injuries • Delay in seeking treatment • Injuries inconsistent with history • Contradictory explanations given by the patient and caregiver • Laboratory findings indicating underdosage or overdosage of medications • Bruises, welts, lacerations, rope marks, burns • Venereal disease or genital infections • Dehydration, malnutrition, decubitus ulcers, poor hygiene • Signs of withdrawal, depression, agitation, or infantile behavior
Physical and Mental Impairment • Recent studies have failed to show direct correlation between patient frailty and abuse, even though it had been assumed that frailty itself was a risk factor for abuse. • Physical and mental impairment nevertheless appear to play an indirect role in elder abuse, decreasing seniors' ability to defend themselves or to escape, thus increasing vulnerability.
Caregiver Stress This theory suggests that elder abuse results from the stress of caring for an elderly patient compounded by stresses from the outside. • alcohol or drug abuse • potential for injury from falls • low income on the part of the abuser • elderly persons' violent verbal behavior • incontinence These all culminate in caregivers' expressions of anger or antagonism toward the elderly person, resulting in violence. Some caregivers manage to endure stresses without becoming abusers, so stress should be seen more as a trigger for abuse than a cause.
Transgenerational Violence • This theory asserts that family violence is a learned behavior that is passed down from generation to generation. • Thus, the child who was once abused by the parent continues the cycle of violence when both are older.
Psychopathology • This theory focuses on a psychological deficiency in the development of the abuser. • Drug and alcohol addiction • Personality disorders • Mental retardation • Dementia • Family members with such conditions are more likely to be primary caretakers for elderly relatives because they are the individuals typically at home due to lack of employment.
WORKUP Lab Studies: Look for evidence of infection, dehydration, electrolyte abnormalities, malnutrition, improper medication administration, and substance abuse in patients who have been abused. • CBC • Chem-7 • Urinalysis • Calcium, magnesium, phosphorus • Serum levels of relevant medications • Urine drug screen • Ethanol level • Pre-albumen
Imaging Studies: • X-rays of relevant body parts - To detect fractures (unusual or pathologic) • Head CT scan - To detect intracranial bleeding as a result of abuse or to detect a possible explanation for injuries (eg, hydrocephalus causing ataxia leading to falls)
MANAGEMENT • Whenever abuse is suspected, the clinician's highest priority is to protect the safety of the elderly person while respecting the person's autonomy. • Mandated reporting is essential at this point.
What is a Mandated Reporter? A mandated reporter is an individual who is required by state law to report situations immediately when they • suspect an adult may have been abused, neglected or exploited, or • is at risk of being abused, neglected or exploited.
Mandated Reporters In most states this is any licensed health care worker or social worker among others. It includes • physicians • nurses • social workers • probably YOU
When Do I Report? • Mandated reporters are required to report situations they encounter while performing their official job duties. • Some states require reporting of an abuse a mandated reporter knows of, regardless of setting. • The report must be made immediately upon becoming aware of the situation of abuse, neglect and/or exploitation.
What Do I Report? • The identity, age, and location of the abused adult. • Any information about the suspected abuse, neglect or exploitation.
WHO DO I CALL? The Adult Protective Services Unit of the Local Department of Social Services in the city or county where the adult resides or in which the abuse, neglect or exploitation occurred. This is the case in VA, NC, and SC.
Other Reporting Requirements • Any reporter who suspects that an adult has died as a result of abuse or neglect must notify the appropriate medical examiner and law enforcement. • Suspected sexual abuse must be reported to social services, who will report it to law enforcement. • Other criminal activity involving abuse or neglect that puts an adult in danger of death or harm must be reported to law enforcement.
Remember!! The Health Insurance Portability and Accountability Act (HIPAA) allows health care providers to release medical records of individuals who are, or are suspected of being, victims of abuse, neglect or exploitation in states that have laws that require the release of such information.
Rights of Mandated Reporters • Immunity from civil and criminal liability • Protection of identity • Permitted to release confidential information without penalty
Penalties for Failure to Report • Large fines are levied for failure to report. • One’s license is in jeapordy in some circumstances. • The court system will determine penalties for failure to tell law enforcement personnel.