Download

1 / 43
430 likes | 451 Views
The Kidney Disease Acronym Spectrum: ARI, CKD, AKI, ARF, and ESRD. Trey La Charité, MD Physician Advisor, Clinical Documentation Integrity Project and Coding University Health Systems Knoxville, TN Cell: 865/250-9625 Office: 865/305-9081 Clachari@mc.utmck.edu. Topic Outline.

E N D
The Kidney Disease Acronym Spectrum: ARI, CKD, AKI, ARF, and ESRD Trey La Charité, MD Physician Advisor, Clinical Documentation Integrity Project and Coding University Health Systems Knoxville, TN Cell: 865/250-9625 Office: 865/305-9081 Clachari@mc.utmck.edu
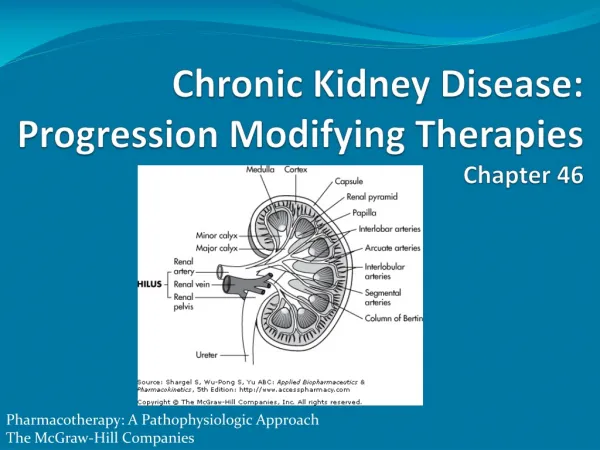
Topic Outline • Basic renal anatomy/physiology • Clinical and CDI implications of BUN & Cr • Renal disease definitions with CDI applications • ARF/AKI • CKD • ARI • ESRD • Emergent HD indications • Query opportunity examples
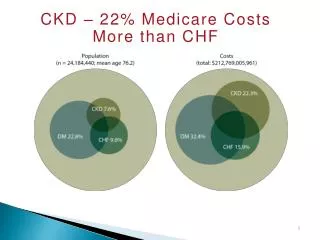
Kidney Facts • Each kidney about size of computer mouse or closed fist • Nephron is functional unit of kidney • Each kidney contains ~ 1 million nephrons • Number of nephrons naturally decreases by ~ 10% every decade of life • Everybody gets CKD if live long enough! • Clinicians monitor blood urea nitrogen (BUN) & serum creatinine (Cr) to assess renal function • Patients may not show any clinical signs of disease until only 20% of nephrons remain
Kidney Structure Nephron
Basic Renal Physiology • Glomerular filtration rate (GFR) = amount of blood filtered through all nephrons in 1 hour • “Normal” GFR (eCrCl) ~125 cc/hr • Ultrafiltrate moves into and through Bowman’s capsule into nephron tubule system: • Ultrafiltrate modified in nephron tubule system via reabsorption, secretion, and concentration • Only 1% of initial ultrafiltrate excreted as urine Proximal convoluted tubule Distal convoluted tubule Loop of Henle
Renal Physiology Facts • Ultrafiltrate in Bowman’s capsule contains everything (BUN & Cr) but cells & large proteins • PCT reabsorbs Na+, Cl-, H20, AAs, glucose, vits • Loop of Henle reabsorbs H20 concentrating fluid • DCT reabsorbs urea back into blood (BUN) • Collecting duct reabsorbs H20 for further fluid concentration & urea into blood (BUN) • Creatinine filtered & secreted in PCT (only 5%–10%), butnot reabsorbed • Normal serum BUN ~ 10–20 • Normal serum creatinine ~ 1.0
What About the BUN/Cr Ratio? • Understanding BUN/Cr ratio significance can lead clinician to potential cause(s) of kidney function abnormalities • Leads CDI personnel to query opportunities for POA indicators, cause & effect relationships, and missed diagnoses • Normal BUN/Cr ratio = 10:1 to 20:1 • In assessing abnormal kidney function, clinicians review the BUN/Cr ratio to discern if lower, equal to, or higher than normal • Helps suggest cause, guide needed workup, and determine best treatment approach
Clinician Kidney Disease Thinking • Clinicians are taught to divide kidney disease into 3 broad categories: • Prerenal = problem occurs before nephron • Intrarenal = problem occurs within nephron • Post-renal = problem occurs after nephron • BUN/Cr ratio suggests which category current kidney problem likely falls into • Knowing which category kidney abnormality falls into can drive your query process
BUN/Cr Ratio Utility for CDI • Prerenal ~ BUN/Cr ratioGREATER than 20:1 • Reduced blood flow equally decreases both BUN & creatinine filtration at glomerulus • However, urea reabsorption in DCT and collecting duct now increases as pumps have longer time to work on slower moving fluid • Therefore, both values rise but BUN rises faster than creatinine increasing their ratio • Additional findings in prerenal pathology • Urine Na+ < 20 • FeNa+ < 1% • FeUrea < 35%
BUN/Cr Query Opportunities • If prerenal (50%–70% of AKI), CDI personnel should then be asking “Why?” • Volume problem • DKA/HHNC • Hemorrhage • Cirrhosis/burns • Vomiting/diarrhea • Perfusion problem • CHF • Shock (septic/cardiogenic)
BUN/Cr Ratio Utility • Intrarenal ~ BUN/Cr ratio LESS than 10:1 • If glomeruli are damaged, BUN & creatinine filtered less but both equally reduced • Nephron tubule damage decreases urea reabsorption as pumps are broken • Serum BUN rises much slower • Therefore, both levels rise but their ratio actually decreases • Additional findings in intrarenal pathology • Urine Na+ > 40 • FeNa+ >> 1% • FeUrea > 50%
BUN/Cr Query Opportunities • If intrarenal (25% of AKI), why? • Vascular • Vasculitis (Wegner’s) – Renal atherosclerosis • Nephrosclerosis – RAS • Glomerular • RPG – IgA nephropathy • Postinfectious – SLE • Membranoproliferative • Tubular • Acute tubular necrosis – Autoimmune • Acute interstitial nephritis – MM
Intrarenal Pathology and CDI • Acute kidney failure codes (584.X) partially differentiated by underlying etiology • 584.9 = Acute kidney failure, unspecified • 584.5 = Acute kidney failure w/ lesion of tubular necrosis • 584.6 = Acute kidney failure w/ lesion of renal cortical necrosis • 584.7 = Acute kidney failure w/ lesion of renal medullary necrosis • 584.8 = Acute kidney failure w/ other specified lesion in kidney • 584.9 is a CC while rest are MCCs
BUN/Cr Ratio Utility • Post-renal ~ BUN/Cr ratio EQUAL TOnormal • “Normal” range = 10:1 to 20:1 • Nephron works fine but urine can’t get out of body due to obstruction distal to kidney • Therefore, both levels rise but rise equivalently preserving a relatively normal ratio between them • Additional findings in post-renal physiology • Renal US or CT scan ABD/Pelvis with significant hydronephrosis proximal to obstruction
BUN/Cr Query Opportunities • If post-renal (5%–10% of AKI), why? • BPH • Prostate CA • Bladder CA • Metastatic malignancy (cervical/ovarian) • Retroperitoneal fibrosis • Retroperitoneal hemorrhage/hematoma • Nephrolithiasis
ARF/AKI and CDI • When a patient’s serum creatinine dramatically rises above their baseline level, it is more than just “dehydration” or “azotemia” or “acute renal insufficiency” • This is “acute renal/kidney failure” • Not “acute on chronic kidney disease” • Must write out what “ARF/AKI” means at least once in the chart! • Auditors may question what ARF or AKI means without writing out acronym one time • ARF/AKI definition revised 8/11 by KDIGO
Acute Kidney Injury Definition • Any rise in serum creatinine of 0.3 mg/dl or more above patient’s baseline ... -Either/Or- 2. Any rise greater than or equal to 1.5 times patient’s baseline serum creatinine • “Baseline” = lowest recorded creatinine value for patient in preceding 3 months www.renal.org/Clinical/GuidelinesSection/AcuteKidneyInjury.aspx* *Note: This was updated in March 2012
ARF/AKI Query Strategy • First, decide/verify whether patient meets criteria of ARF/AKI • If no, yet clinician has called this in chart, will need clarification prior to coding • Coders not allowed to question physicians’ judgment while post-discharge auditors are allowed • If yes, go to next step • Second, calculate the BUN/Cr ratio • Is problem pre-, intra-, or post-renal? • Third, is the urinalysis helpful? • With this information, is there now opportunity to further clarify why patient has ARF/AKI?
What About the Urinalysis? • Prerenal • Hyaline casts • Intrarenal • Proteinuria • Cells (WBCs & RBCs) • Cell casts: • WBC (AIN) • RBC (glomerulonephritis) • Epithelial (ATN) • Post-renal • Benign/no significant abnormalities • Hematuria
Current ARF/AKI Coding • Per KDIGO, “acute renal failure” terminology to be replaced by “acute kidney injury” • Problem: “AKI” currently codes to “ARF” • Therefore, physicians should not document AKI unless they truly mean ARF • Watch for clinicians using AKI to describe any acute renal abnormality even if does not meet ARF criteria • Some physicians will adopt this new terminology regardless of coding implications • May increase need for query clarifications, so do not report ARF when not actually present
Future ARK/AKI Coding? • Presently, no documentation benefit for physicians documenting stage of AKI • Hopefully … ICD-9 or ICD-10 codes will be created for AKI stages • Suspect … Stages 1 & 2 will be CCs while Stage 3 will be an MCC • Start medical staff education of stages when AKI codes definitively arrive • Teaching new failure definitions tough enough without confusing issue with stages
Chronic Kidney Disease Def: Presence of kidney damage or decreased kidney function persisting for at least 3 months regardless of cause • Stage I • Stage II • Stage III GFR = > 90 ml/min GFR = 60–89 GFR = 30–59 • Stage IV • Stage V GFR = 15–29 CC GFR < 15 CC (but no HD/PD)
Chronic Kidney Disease • In order to properly stage CKD, physicians must either calculate CrCl or have it provided for them • Reduced credit given if physician documents “CKD” only without stage • eCrCl estimates GFR via Cockcroft-Gault eq X 0.85 for women (140 - patient’s age) x patient’s wt in Kgs eCrCl = 72 x patient’s baseline serum creatinine patient’s ideal weight = 60 Kgs for women and 70 Kgs for men
CKD Query Opportunities • Most important determinants of Cockcroft-Gault equation estimation: • Patient’s age • Patient’s serum creatinine • Serum creatinine greater effect than age • Calculate CrCl for anybody with ... • Serum creatinine > 1.0 • Age of 50 years or older regardless of serum creatinine level • Why?
What if Acute Rise But Not ARF? • In the acute setting, what does one call the “no-man’s land” between a patient’s baseline creatinine and ARF/AKI? Patient’s baseline creatinine (normal or CKD) ? ARF AKI Increasing serum creatinine
No ‘Great’ Answers • “Azotemia” or “uremia” = 790.6, Other abnormal blood chemistry • “Dehydration” = 276.51 • Not accurate for creatinine rises due to intra- or post-renal etiologies • “Acute nephropathy” = 580.9, Acute glomerulonephritis with unspecified pathologic lesion in kidney • “Acute renal insufficiency” = 593.9, Unspecified disorder of kidney and ureter
End-Stage Renal Disease • Failure of kidneys to perform functions necessary to support daily life • Usually occurs when less then 10% of renal function remains • Patients cannot survive without routine dialysis or a kidney transplant • Patients qualify for permanent dialysis when their measured CrCl is 10 mg/dl or less • Query opportunity for ESRD when here • Your nephrologists may start preparing patient for HD/PD when CrCl = 15mg/dl • ESRD (585.6) is an MCC
Emergent HD Query Opportunities • Indications for emergent dialysis: A = Acidosis E = Electrolytes (i.e., hyperkalemia causing cardiac arrhythmias) I = Ingestion (beware of psychiatric codes as principal dx) O = Overload (Is there really acute CHF?) U = Uremia (not really done anymore) Y = Why?Why not because nobody understands nephrology or nephrologists!
Example #1 • 48 yo WF comes to ED with complaints of fever, chills, cough w/ green sputum, myalgias, and weakness. She is tachycardic w/ T = 102.7. She is hypotensive & requires 4 liters IVF to normalize BP. Initial WBC = 28.7. Initial workup reveals sepsis due to multilobar pneumonia. Patient did notice her urine had been very dark. Initial BUN & Cr are 32 & 3.8. Last recorded BUN & Cr were 19 & 0.8 in PCP’s office 2 months ago. UA reveals large amount of protein and numerous epithelial cell casts. BUN & Cr almost normalize by time of discharge.
Example #1 • Patient initially admitted to ICU for “sepsis” and “acute renal failure.” • Does the patient have acute renal failure? • Absolutely! 1.5 x 0.8 = 1.2 • What’s the BUN/Cr ratio? • 32/3.8 = 8.42 • Does the urinalysis help? • Epithelial cell casts and large proteinuria consistent with ATN • Query opportunity for ARF due to ATN (POA) potentially giving case an MCC = Intrarenal
Example #2 • 87 yo WM w/ Alzheimer’s dementia, CHF, CAD, & PVD sent to ED from NH for lethargy & unresponsiveness. Initial workup reveals Na+= 167, Cl- = 118, K+ = 5.5, BUN = 89, Cr = 2.8. Lowest recorded BUN & Cr = 29 & 2.1 at recent discharge for diastolic CHF exacerbation 6 weeks earlier. CBC essentially WNL while had always been anemic during previous admissions. Urinalysis significant for numerous hyaline casts. Patient aggressively hydrated and BUN & Cr return to his baseline. Patient eventually discharged to a different nursing home.
Example #2 • Patient initially admitted for “acute renal failure.” • Does the patient have acute renal failure? • NO! 2.1 + 1.0 =3.1 • What’s the BUN/Cr ratio? • 89/2.8 = 31.79 • Does the urinalysis help? • Hyaline casts consistent with prerenal cause • Clarification opportunity for ARI on CKD stage 4 possibly preventing an incorrect coding submission of ARF = Prerenal
Example #3 • 63 yo WM comes to ED for painful urination, difficulty initiating stream, hematuria, weakness, & 4 months wt. loss w/out effort. Not seen physician since 1976. CT scan of urinary tract reveals bilateral hydronephrosis w/ markedly enlarged & necrotic-appearing prostate w/ pelvic lymphadenopathy. Initial BUN & Cr noted to be 55 & 3.3. Foley catheter insertion results in significant diuresis & eventual normalization of BUN & Cr. UA WNL except for hematuria. After biopsy, principal diagnosis established as “metastatic prostate cancer” & radical prostatectomy is performed.
Example #3 • Primary service repeatedly documents “obstructive uropathy” to describe renal function. • Does the patient have acute renal failure? • Absolutely! BUN & Cr normalized • What’s the BUN/Cr ratio? • 55/3.3 = 15.71 • Does the urinalysis help? • Hematuria only not much help • Query opportunity for acute renal failure (POA) potentially giving case a CC = Post-renal
Example #4 • 27 yo AA male comes to ED complaining of hard & painful inguinal lesions, recurrent fevers w/ chills, weakness, & fatigue. Initial VS reveal BP = 88/45, HR = 113, T = 101.9, RR = 28, RA O2 sat = 98%. Initial BUN & Cr = 31 & 1.4, which improve to 21 & 1.1 w/ hydration. Patient diagnosed w/ sepsis & requires several abscess I&D procedures. Blood cxs & abscess cxs repeatedly grow streptococcal species despite broad spectrum ABX. On hospital day 9, BUN & Cr start to rise. By day 13, BUN & Cr = 34 & 4.3 despite aggressive IVF & numerous medication adjustments.
Example #4 • Does the patient have acute renal failure? • Absolutely! 1.1 x 1.5 = 1.65 • What’s the BUN/Cr ratio? • 34/4.3 = 7.9 • Is the urinalysis helpful? • Proteinuria consistent w/ intrarenal pathology • ASO titer returns positive & renal biopsy reveals postinfectious glomerulonephritis • Query opportunity for ARF & acute post-streptococcal glomerulonephritis (POA) potentially giving case 1 CC & 1 MCC = Intrarenal
Example #5 • 67 yo WM comes to ED w/ complaints of SOB, swelling, & weakness. Neighbor found him after being in shower for 6 hours because too weak to get out. Patient has severe anasarca w/ BUN & Cr of 94 & 2.9. UA w/ 3–5 hyaline casts. CXR shows pulmonary edema & ECHO reveals EF ~ 15% w/ global hypokinesis. CHF medication optimization & aggressive IV diuretic regimen do not produce significant urine output. Natricor & Bumex drip finally produce results. Patient also hypotensive throughout hospitalization. Patient goes home w/ BUN & Cr down to 53 & 1.7.
Example #5 • Patient initially admitted for “anasarca” only. • Does the patient have acute renal failure? • Absolutely! 1.7 x 1.5 = 2.55 • What’s the BUN/Cr ratio? • 94/2.9 = 32.4 • Does the urinalysis help? • Hyaline casts consistent with prerenal cause • Query opportunities for establishing acute systolic CHF exacerbation (POA) as principal diagnosis and for ARF & cardiogenic shock potentially giving case 1 CC & 1 MCC = Prerenal
Questions? In order to receive your continuing education certificate for this program, you must complete the online evaluation which can be found in the continuing education section at the front of the workbook.