Download

1 / 35
360 likes | 718 Views
Basic Approach to cyanosis in infancy. Cardiology Red Cross Children's Hospital. “You do not really understand something unless you can explain it to your grandmother.” . Dr. Albert Einstein. Most common reason for referral to cardiologist in the 1 st years of life: Heart Murmur Cyanosis

E N D
Basic Approach to cyanosis in infancy Cardiology Red Cross Children's Hospital
“You do not really understand something unless you can explain it to your grandmother.” Dr. Albert Einstein
Most common reason for referral to cardiologist in the 1st years of life: • Heart Murmur • Cyanosis • Congestive Cardiac Failure • Arrythmias • Abnormal CXR • Abnormal ECG
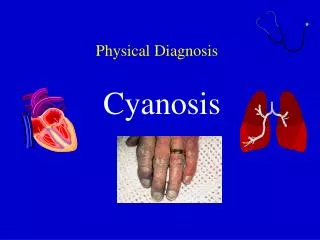
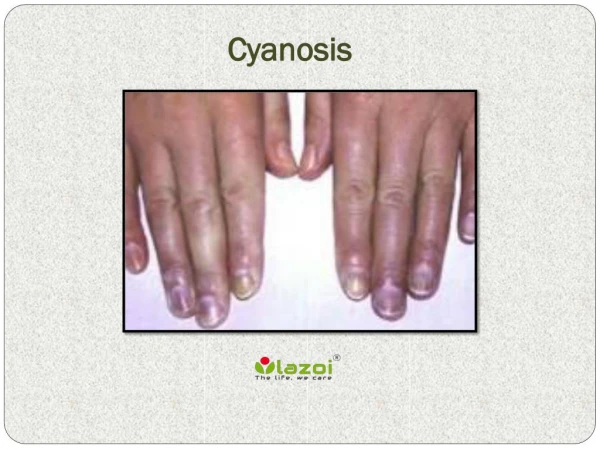
Cyanosis(form the Greek word meaning dark blue) • What is cyanosis? • Blue discolouration of lips / tongue / extremeties • Oxygenated Hb is bright red • Reduced Hb is blue / purple • Cyanosis is dependent upon the absolute concentration of reduced Hb. • TcSaO2<85% OR > 3g deoxygenated Hb • If present through the entire body= CENTRAL CYANOSIS • If present only in the extremeties = PERIPHERAL CYANOSIS
Making the diagnosis • Clinically: • Early detection in newborns is essential • May be difficult to see in dark skinned individuals – tip of tongue • Good lighting essential • Thermo-neutral environment • Is the child distressed/any other signs of cardiac abnormalities?? • Does the blueness fade on pressure? • Is the child cold / poorly perfused
If in doubt – Saturation with pulse oximeter and/or arterial blood gas: • Normal TcSaO2 in newborn in room air is 92% • Normal PaO2 in newborn is >60mmHg (>8Kpa)
Transcutaneous Saturation measurement • Uses light absorption at a given wavelength • measures bound O2 • assumes a normal haemoglobin molecule • Sat of 94% - equivalent to Sa02 of 90% • Misses bradyarrythmias • Completely inaccurate below 70% (beware of nail polish!!!!) • Ear best in a shocked patient
In a nutshell….. • Respiratory disease • Shock • metabolic derangement • hypoglycaemia, hypothermia • congenital heart disease • methaemoglobinaemia • persistent foetal circulation
Steps in the management of cyanotic newborns: • CHEST XRAY: • May reveal pulmonary cause • May hint to the presence or absence of cardiac lesion • ARTERIAL BLOOD GAS IN ROOM AIR: • Confirm or reject cyanosis • Elevated pCO2 suggests pulmonary or CNS cause • LOW pH in severe shock, sepsis, severe hypoxaemia • HYPEROXIA TEST: • ECG: • If cardiac disease suspected – will give clue to diagnosis • PROSTAGLANDIN E1: • If heart lesion suspected that is ductus dependent (eg pulmonary atresia,Tetralogy of Fallot, TGA, Coarctation of the aorta)
Asphyxia CNS (hypoventilation) Hb abnormalities Metabolic causes CXR Pulmonary/Cardiac • Assessment of cyanosis ABG Hyperoxia test Cardiac vs Pulmonary cause Septic Screen Blood glucose Sepsis Hypoglycaemia Polycythaemia ECG Echocardiogram Cardiac Cause PPHN
The Chest X Ray • “classical” patterns - rare • better use is to judge pulmonary flow • oligaemia - dark lung fields - tetralogy • plethora - increased flow - mixers • use to side the arch • visceral situs in complex forms
The hyperoxia test • Cyanosis confirmed with arterial oxygen measurement • to differentiate between respiratory and cardiac causes of cyanosis • administer oxygen at the highest concentration possible (head box) • blood gas from Right radial artery • Wait for 15 minutes – repeat ABG • pO2 < 150 mm Hg (20 kPa) - cardiac • pO2 > 250 mm Hg (33 kPa) - respiratory
Failures of the Hyperoxia test • Cyanotic heart defect with large pulmonary blood flow (eg TAPVD) – pO2 may rise with O2 administration. • Massive intrapulmonary shunts but a normal heart (eg PPHN, AVM) may not raise the pO2 with oxygen – pO2 wont rise with O2. • Response to oxygen inhalation must be interpreted in the light of the clinical picture
BEFORE REFERRAL TO CARDIOLOGIST – ATTEMPT TO MAKE A REASONABLE DIAGOSIS
CXR Reduced Pulmonary Blood flow Increased Pulmonary Blood flow ECG Tetralogy RVH RVH TAPVD PAtresia Tric atresia LVH LVH TGA DTGA Truncus CVH
Explanation of a few common cyanotic congenital heart defects
TETRALOGY OF FALLOT Infundibular “PS” Aorta overrides septum LA VSD RA LV RV RVH
“PALLIATED” TETRAOGY Blalock-Taussig shunt LA RA LV RV
TETRALOGY OF FALLOT Ejection systolic murmur Single S2 NO RV heave RV HYPERTROPHY INFUNDIBULAR STENOSIS VSD NO CYANOSIS AORTIC OVERRIDE MILD CYANOSIS
TETRALOGY OF FALLOT ‘HYPERCYANOTIC SPELL’ Tachypnoea NO ejection systolic murmur Death CYANOSIS POSITIVE FEEDBACK ACIDOSIS
TRANSPOSITION OF THE GREAT ARTERIES Pulmonary Artery from LV Aorta from RV LA RA LV RV
TGA LAENLARGEMENT LVENLARGEMENT RV LV Two separate parallel circuits Incompatible with life No murmurs Aorta PA SEVERE CYANOSIS CCF
TGA IVC Rashkind atrial septostomy Followed by : Arterial switch or Mustard operation PDA
TRICUSPID ATRESIA LA VSD RA LV Atretic TV
TRUNCUS ARTERIOSUS Aorta Pulmonary artery “Truncus” VSD RA LV RV
after referral? • ECG can give clues to the diagnosis • echocardiography - main diagnostic tool • catheterisation - particularly to assess pulmonary artery structure and size • balloon septostomy in TGA • use of IV prostaglandin to keep the duct open • surgery
Pre Muscle resection Post Muscle resection