Download
1 / 1
20 likes | 172 Views
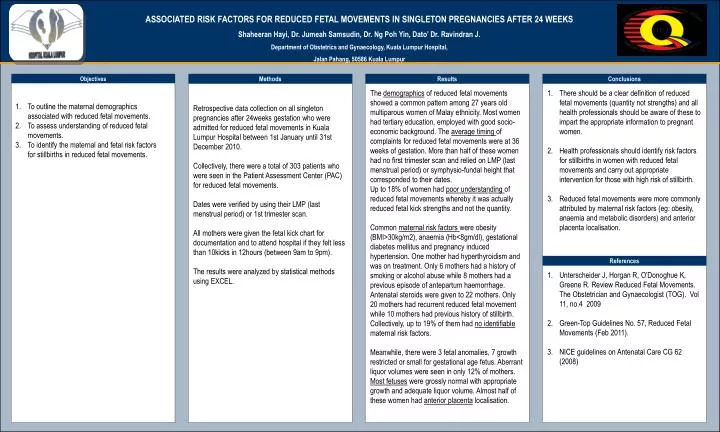
ASSOCIATED RISK FACTORS FOR REDUCED FETAL MOVEMENTS IN SINGLETON PREGNANCIES AFTER 24 WEEKS Shaheeran Hayi, Dr. Jumeah Samsudin, Dr. Ng Poh Yin, Dato’ Dr. Ravindran J. Department of Obstetrics and Gynaecology, Kuala Lumpur Hospital, Jalan Pahang, 50586 Kuala Lumpur. OPTIONAL LOGO HERE.

E N D
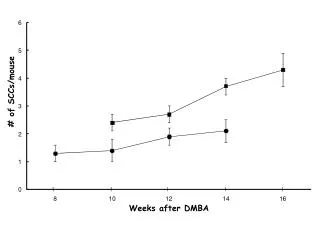
ASSOCIATED RISK FACTORS FOR REDUCED FETAL MOVEMENTS IN SINGLETON PREGNANCIES AFTER 24 WEEKS Shaheeran Hayi, Dr. Jumeah Samsudin, Dr. Ng Poh Yin, Dato’ Dr. Ravindran J. Department of Obstetrics and Gynaecology, Kuala Lumpur Hospital, Jalan Pahang, 50586 Kuala Lumpur OPTIONALLOGO HERE OPTIONALLOGO HERE Objectives Methods Results Conclusions • Retrospective data collection on all singleton • pregnancies after 24weeks gestation who were • admitted for reduced fetal movements in Kuala • Lumpur Hospital between 1st January until 31st • December 2010. • Collectively, there were a total of 303 patients who • were seen in the Patient Assessment Center (PAC) • for reduced fetal movements. • Dates were verified by using their LMP (last • menstrual period) or 1st trimester scan. • All mothers were given the fetal kick chart for • documentation and to attend hospital if they felt less • than 10kicks in 12hours (between 9am to 9pm). • The results were analyzed by statistical methods • using EXCEL. The demographics of reduced fetal movements showed a common pattern among 27 years old multiparous women of Malay ethnicity. Most women had tertiary education, employed with good socio-economic background. The average timing of complaints for reduced fetal movements were at 36 weeks of gestation. More than half of these women had no first trimester scan and relied on LMP (last menstrual period) or symphysio-fundal height that corresponded to their dates. Up to 18% of women had poor understanding of reduced fetal movements whereby it was actually reduced fetal kick strengths and not the quantity. Common maternal risk factors were obesity (BMI>30kg/m2), anaemia (Hb<8gm/dl), gestational diabetes mellitus and pregnancy induced hypertension. One mother had hyperthyroidism and was on treatment. Only 6 mothers had a history of smoking or alcohol abuse while 8 mothers had a previous episode of antepartum haemorrhage. Antenatal steroids were given to 22 mothers. Only 20 mothers had recurrent reduced fetal movement while 10 mothers had previous history of stillbirth. Collectively, up to 19% of them had no identifiable maternal risk factors. Meanwhile, there were 3 fetal anomalies, 7 growth restricted or small for gestational age fetus. Aberrant liquor volumes were seen in only 12% of mothers. Most fetuses were grossly normal with appropriate growth and adequate liquor volume. Almost half of these women had anterior placenta localisation. • There should be a clear definition of reduced fetal movements (quantity not strengths) and all health professionals should be aware of these to impart the appropriate information to pregnant women. • Health professionals should identify risk factors for stillbirths in women with reduced fetal movements and carry out appropriate intervention for those with high risk of stillbirth. • 3. Reduced fetal movements were more commonly attributed by maternal risk factors (eg: obesity, anaemia and metabolic disorders) and anterior placenta localisation. • 1. To outline the maternal demographics associated with reduced fetal movements. • 2. To assess understanding of reduced fetal movements. • To identify the maternal and fetal risk factors for stillbirths in reduced fetal movements. References • Unterscheider J, Horgan R, O’Donoghue K, Greene R. Review Reduced Fetal Movements. The Obstetrician and Gynaecologist (TOG). Vol 11, no.4 2009 • Green-Top Guidelines No. 57, Reduced Fetal Movements (Feb 2011). • NICE guidelines on Antenatal Care CG 62 (2008)