Download
1 / 19
200 likes | 551 Views
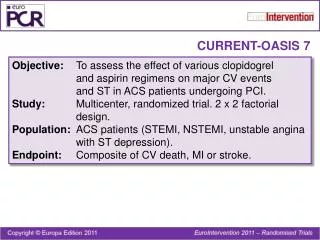
OASIS-7. CURRENT OASIS 7: A 2X2 Factorial Randomized Trial of Optimal Clopidogrel and Aspirin Dosing in Patients with ACS Undergoing an Early Invasive Strategy with Intent For PCI. Shamir R. Mehta on behalf of the CURRENT Investigators.

E N D
OASIS-7 CURRENT OASIS 7: A 2X2 Factorial Randomized Trial of Optimal Clopidogrel and Aspirin Dosing in Patients with ACS Undergoing an Early Invasive Strategy with Intent For PCI Shamir R. Mehta on behalf of the CURRENT Investigators Disclosures: CURRENT OASIS 7 was funded by a grant from sanofi-aventis and Bristol Myers Squibb. All data were managed independently of the sponsor at the PHRI, McMaster University and the trial was overseen by an international steering committee of experts.
Background • Clopidogrel • Clopidogrel 300 mg followed by 75 mg daily reduces major CV events across the spectrum of ACS and PCI • Recent data suggest that doubling the loading and maintenance doses of clopidogrel results in a higher and more rapid antiplatelet effect • Aspirin • Dose of ASA varies between Europe and North America • No large-scale RCT’s have compared high (300-325 mg) versus low (75-100) dose aspirin in patients with ACS undergoing PCI
Benefits of Antiplatelet Therapy in ACS are Greater in Patients Undergoing PCI 1. Mehta SR, et al. Lancet 2001; 358(9281):527-33. 2. Fox KAA, et al. Circulation 2004;110:1202-8 3. Sabatine MS, et al. JAMA 2005; 294(10):1224-32. 4. Chen ZM Lancet 2005;366:1607-21 4. Boersma E et al. Lancet 2002; 359:189 5. Wiviott S et al. N Engl J Med 2007; 357: 2001–15.
Study Design, Flow and Compliance • 25,087 ACS Patients (UA/NSTEMI 70.8%, STEMI 29.2%) • Planned Early (<24 h) Invasive Management with intended PCI • Ischemic ECG Δ (80.8%) or ↑cardiac biomarker (42%) Randomized to receive (2 X 2 factorial): CLOPIDOGREL: Double-dose(600 mg then150 mg/d x 7d then 75 mg/d) vsStandard dose (300 mg then 75 mg/d) ASA: High Dose (300-325 mg/d) vsLow dose(75-100 mg/d) Angio 24,769 (99%) PCI 17,232 (70%) No PCI 7,855 (30%) No Sig. CAD 3,616 CABG 1,809 CAD 2,430 Compliance: Clop in 1st 7d (median) 7d 7 d 2 d 7d Efficacy Outcomes: CV Death, MI or stroke at day 30 Stent Thrombosis at day 30 Safety Outcomes:Bleeding (CURRENT defined Major/Severe and TIMI Major) Key Subgroup:PCI v No PCI Complete Followup 99.8%
ASA Dose ComparisonPrimary Outcome and Bleeding GI Bleeds: 30 (0.24%) v 47 (0.38%), P=0.051 No other significant differences between ASA dose groups
Clopidogrel Dose Comparison • 2 Significant Interactions: • PCI v No PCI (P=0.016) • ASA dose (P=0.043)
Clopidogrel: Double vs Standard DosePrimary Outcome and Components
Clopidogrel Double vs Standard DoseBleeding Overall Population 1ICH, Hb drop ≥ 5 g/dL (each unit of RBC transfusion counts as 1 g/dL drop) or fatal 2Severe bleed + disabling or intraocular or requiring transfusion of 2-3 units 3Fatal or ↓Hb ≥ 5 g/dL, sig hypotension + inotropes/surgery, ICH or txn of ≥ 4 units
Clopidogrel: Double vs Standard Dose Definite Stent Thrombosis (Angio confirmed) Clopidogrel Standard Dose 0.012 42% RRR 0.008 Cumulative Hazard Clopidogrel Double Dose 0.004 HR 0.58 95% CI 0.42-0.79 P=0.001 0.0 0 3 6 9 12 15 18 21 24 27 30 Days
Clopidogrel: Double vs Standard DoseMajor Efficacy Outcomes in PCI Patients
Clopidogrel: Double vs Standard Dose Primary Outcome: PCI Patients CV Death, MI or Stroke Clopidogrel Standard 15% RRR 0.04 Clopidogrel Double 0.03 Cumulative Hazard 0.02 HR 0.85 95% CI 0.74-0.99 P=0.036 0.01 0.0 0 3 6 9 12 15 18 21 24 27 30 Days
Clopidogrel Double vs Standard DoseBleeding PCI Population 1ICH, Hb drop ≥ 5 g/dL (each unit of RBC transfusion counts as 1 g/dL drop) or fatal 2Severe bleed + disabling or intraocular or requiring transfusion of 2-3 units 3Fatal or ↓Hb ≥ 5 g/dL, sig hypotension + inotropes/surgery, ICH or txn of ≥ 4 units
Clopidogrel: Double v Standard DosePCI Cohort Subgroups CV Death, MI or Stroke MI or Stent Thrombosis 2N Std % Double % Intxn P Std % Double % Intxn P Overall 17232 4.5 3.9 3.7 3.0 NSTEMI/UA 10886 4.2 3.6 3.6 3.1 0.805 0.248 STEMI 6346 5.0 4.2 4.0 2.8 Male 13009 4.1 3.6 3.5 3.0 0.419 0.148 Female 4223 5.8 4.6 4.6 3.0 Age <= 65 yrs 10975 3.0 2.7 2.9 2.2 0.702 0.418 Age > 65 yrs 6257 7.1 6.0 5.2 4.4 Non-Diabetic 13400 4.2 3.6 3.6 2.8 0.836 0.567 Prev Diabetic 3831 5.6 4.9 4.1 3.6 No Inhosp GPIIb/IIIa 12288 3.9 3.5 3.1 2.5 0.465 0.894 GPIIb in hosp 4936 6.0 4.7 5.2 4.1 No Prot Pump Inhib 7675 3.8 3.2 3.1 2.3 0.408 0.613 Prot Pump Inhib 5557 5.7 4.2 4.8 3.3 Non-smoker 10845 4.9 4.6 3.9 3.5 0.045 0.050 Current Smoker 6380 3.8 2.6 3.4 2.1 ASA Low 8620 4.2 4.3 3.6 3.2 0.024 0.191 ASA High 8612 4.8 3.5 3.8 2.7 Double Dose Better Std Dose Better Double Dose Better Std Dose Better 0.50 1.50 0.50 1.50
Definite Stent Thrombosis in 4 Groups (Angiographically Proven) C Standard, A Low 0.012 C Standard, A High C Double, A Low 0.008 Cumulative Hazard C Double, A High 0.004 0.0 0 3 6 9 12 15 18 21 24 27 30 Days
ConclusionsClopidogrel Dose Comparison • Double-dose clopidogrel significantly reduced stent thrombosis and major CV events (CV death, MI or stroke) in PCI. • In patients not undergoing PCI, double dose clopidogrel was not significantly different from standard dose (70% had no significant CAD or stopped study drug early for CABG). • There was a modest excess in CURRENT-defined major bleeds but no difference in TIMI major bleeds, ICH, fatal bleeds or CABG-related bleeds.
ConclusionsASA Dose Comparison • No significant difference in efficacy or bleeding between ASA 300-325 mg and ASA 75-100 mg.
Clinical Implications • For every 1,000 patients with ACS receiving PCI, using double-dose clopidogrel for 7 days instead of standard dose will prevent an additional 6 MI’s and7 stent thromboses with an excess of 3 severe bleeds and no increase in fatal, CABG-related or TIMI major bleeds. • Patients not undergoing PCI should continue to use the standard dose regimen of clopidogrel.
Acknowledgements CURRENT Investigators from 597 sites in 39 countries Steering Committee Sponsors Project Office DSMB Adjudication Committee Consultant: R. Peto