Download

1 / 39
580 likes | 2.01k Views
Distal radius fracture. June 17 2009 Asim Makhdom. Epidemiology. Frequency 17% of all ER visits . Distal radial fractures account for 1/6 of all fractures seen in the ED Race: No racial preferences have been reported. Age Bimodal age distribution:

E N D
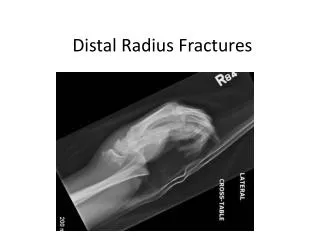
Distal radius fracture June 17 2009 Asim Makhdom
Epidemiology Frequency • 17% of all ER visits . • Distal radial fractures account for 1/6 of all fractures seen in the ED • Race: No racial preferences have been reported.
Age Bimodal age distribution: Peaks at ages 5-14 years and at ages 60-69 years. Elderly patients extra-articular, metaphyseal Young patients intra-articular fractures with joint surface displacement. Gender In older postmenopausal women, female-to-male ratio 4:1 but In adolescent boys and girls, the ratio is 3:1
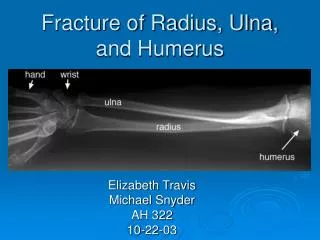
Anatomy • articular plateau upon which carpus rests • gives origin of ligament which wrist joint stability rests • also forms articulation with ulnar head combined with TFCC • 3 concave articular facets-scaphoid fossa-lunate fossa-sigmoid notch
TFCC major stabiliser of ulnar carpus & radioulnar joint • normal wrist movement -150 degree of motion (flex/ext) • -50 deg radial/ulnar deviation-150 deg pron/sup • axial load-80% radius -20% TFCC
Mechanism Of Injury Low energy trauma: FOOSH In young adult, injury usually is as result of high energy trauma & results in comminuted, intraarticular injuries Tension on the volar cortex, comminution of the dorsal cortex, and ligamentous injury
Diagnosis • History • Physical exam, look for other injury injury should be evaluated for:- • open/closed • degree of soft tissue injury • neurovascular injury- median nerve injury common • Imaging Wrist PA, Lat, and oblique AP and lat. Of the contralateral wrist Ct scan
Radiographic Assessment • radial inclination • volar tilt • radial length • Any intra-articular gap or step
Specific fracture types • Colle's:Dorsal displacement (Abraham Colles (1773-1843), Irish surgeon and anatomist)Smith's:Volar displacement (Robert William Smith (1807-1873), Irish surgeon)Barton's:Radial rim fracture with dislocation of the radiocarpal joint (can be dorsal or volar); John Rhea Barton (1794-1871) American surgeon.Chauffeur's:Radial styloid
Classifications • Classification system must consider type ,displacement and severity of fracture • should serve as basis for treatment & prognosis • studies have shown that there is little interobserver agreement
Andersen et al compared the Frykman, Melone, Mayo, and AO/ASIF classification systems and concluded that a low degree of intraobserver and interobserver agreement exists in each of these 4 systems.
Treatment Goals pain free, mobile and stable wrist. • Anatomical reduction should be the goal Howard,1989.
Criteria for acceptable reduction Graham1997(Jaaos) 1_Radial shortening less than 5 mm at the distal radioulnar joint (DRUJ) compared with the contralateral wrist. 2_Radial inclination of more than 15° on a posteroanterior (PA) image.
3_Sagittal tilt on the lateral projection between 15° dorsal tilt and 20° volar tilt. • 4_Intra-articular fracture step-off less than 1-2 mm of the radiocarpal joint • Jupiter et al. 2mm or more of articular incongruity led to post-traumatic arthritis
Predictors of stability • Associated Ulnar styliod # • Age of the patient • Extent of metaphyseal comminution • Redisplacement after closed reduction is a predictor of instability and repeated manipulation is unlikely will result in successful radiological outcome
Treatment options • Closed reduction and immobilization • Closed reduction and Percutaneous pinning • External fixation • Arthroscopically assisted reduction and Ex. Fixation of intraarticular fracture. • ORIF with plate fixation • Bone grafting
I. Nonarticular/ undisplaced • II Nonarticular/ displaced A.reducible/stable B.reducible/unstable C.Irreducible/stable • IIIArticular/ undisplaced • -cast immobilisation • -cast immobilisation-percutaneous pins-ORIF/ex fix • -cast immobilisation/ percutaneous pins
IV Articular,displacedA.reducible,stableB.reducible,unstableC.irreducibleD.complex • -closed reduction & K wires-A/A +/- ex fix-ORIF or ex fix & K wires-ORIF/ex fix & wires+ bone graft
Complications Malunion/ non union DRUJ Complicatios ( Incongruent DRUJ) Neurological Injuries Medial, Ulnar, Complex regional pain syndrome Tendon injuries Infection.
TREATMENT COMPARSIONWHERE IS THE EVEDINCE?? • major questions remain:- • (1) Is ex/fix or percutaneous pin fixation a better interventionthan CR when evaluated with validated outcome measures? • (2) How does ORIF compare with ex/fix and percutaneous pin fixation or even CRand cast immobilization?
(3) Is there a particular techniquefor each treatment modality that provides superior results? • (4) As most recent studies include only a maximum of two yearsof follow-up, do the results of treatment endure over the longterm?
Recent randomized, controlled trials have begun to clarify someof these questions!!
Percutanous pin or closed reduction?? • Abela M et al. JBJS2005 • In a study of 57 patients, radiographic parametersafter percutaneous pin fixation IN unstable extra-articular # were found to be significantlybetter than those after closed reduction (p < 0.05); however,there was no difference in SF-36 scores.
Bridging ex/fix or CR?? • YOUNG CF et al2003(J hand S) A series of 85 patients demonstratedstatistically equivalent Gartland and Werley functional scoresafter seven years of follow-up; however, radiographic measureswere significantly better in the external fixation group (p< 0.001).
Kreder et al.(JOT)2006 .When validated outcome scores were used to comparespanning external fixation with closed reduction and cast immobilizationof metaphyseal displacment(DRF) without joint incongruity in 113patients, SF -36bodily pain scores and (MFA) scores at two years favored external fixation.
Augmented external fixation versus percutaneous pinning and casting for unstable fractures of the distal radius?? Harley et al. 2004(JHS) similar validated outcome scores and functionaloutcomes at one year, the patients treated with ex/fixdemonstrated better articular congruity on radiographic follow-up.
Indirect reduction and percutaneous fixation versus open reduction and internal fixation for displaced intra-articular fractures of the distal radius • Kreder et al. 2005(JBJS) • was compared in 179 patients althoughMFA and SF-36 scores at two years were statistically equivalent betweenthe groups, EX/FIX yielded better outcomes at thesix-month interval.
Comparison of External and Percutaneous Pin Fixation versus Plate Fixation for Intra-articular Distal Radial Fractures • Frankie leung et al. 2008(JBJS)At the time of 24 month follow-up, the resultsfor the plate fixation group were significantly better thanthose for the external fixation and percutaneous pin fixationgroup according to the Gartland and Werley point system (p =0.04) and the radiographic arthritis grading system (p = 0.01).The difference was especially notable among patients with AOgroup-C2 fractures.
Bridging external fixation and supplementary Kirschner-wire fixation versus volar locked plating for unstable fractures of the distal radius • K. Egol et al 2008(JBJS) • No clear advantage could be demonstrated with either treatmentbut fewer re-operations were required in the external fixationgroup.
BRIDGING VERSUS NON-BRIDGING EXTERNAL FIXATION ?? • M.McQueen1998(JBJS) noticed Non-bridging external fixation is the treatment of choice forunstable fractures of the distal radius which have sufficientspace for the placement of pins in the distal fragment.