Download
1 / 4
40 likes | 261 Views
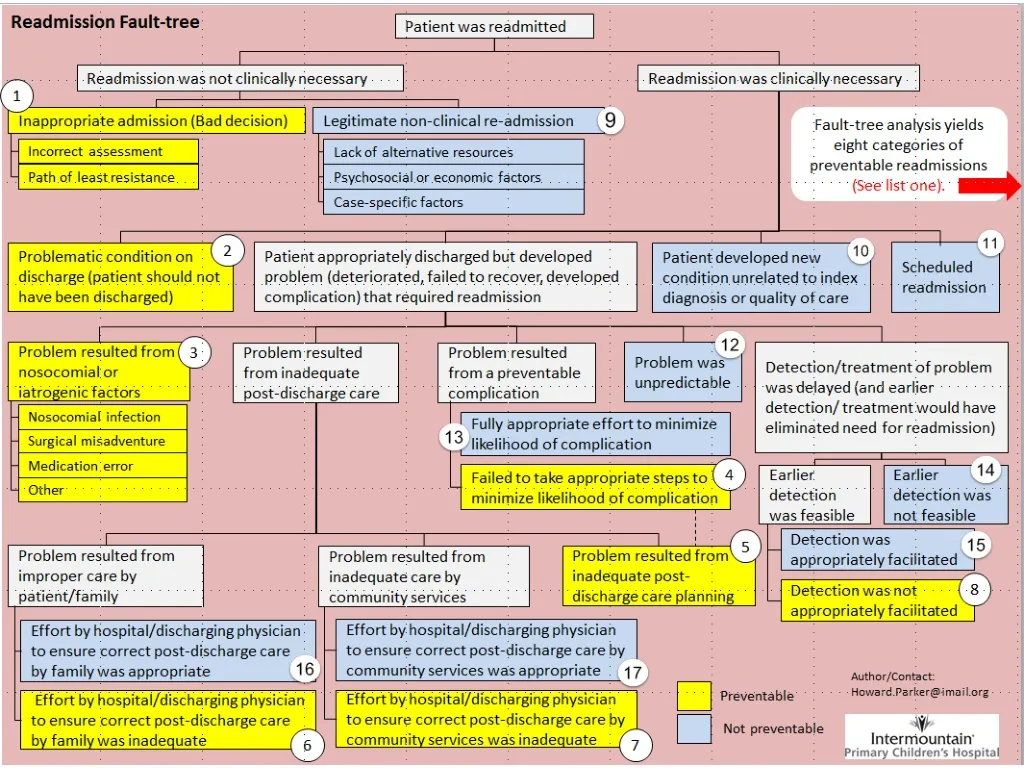
List One: Categories of Preventable Readmissions. 5. Substandard post-discharge care planning . Readmitted because of substandard post-discharge care that was attributable to inadequate care planning on the part of the hospital. 1. Unnecessary readmission .

E N D
List One: Categories of Preventable Readmissions 5. Substandard post-discharge care planning. Readmitted because of substandard post-discharge care that was attributable to inadequate care planning on the part of the hospital 1. Unnecessary readmission. Decision to readmit was incorrect; clinical condition did not warrant readmission and there were no other legitimate factors requiring readmission. 2. Inappropriate discharge. Readmitted because decision to discharge was incorrect; patient was too sick or insufficiently stable to be discharged. 6. Failure to facilitate care by family. Readmitted because thehospital failed to appropriately equip the family to perform post-discharge care 3. Nosocomial/iatrogenic issues. Readmitted for deterioration caused by nosocomial or iatrogenic issues that occurred prior to discharge (e.g., nosocomial infection, surgical misadventure, medication error) 7. Failure to facilitate care by community. Readmitted because of failure of hospital to appropriately facilitate post-discharge care by the outpatient medical community 4. Failure to mitigate known complications. Readmitted because hospital did not take steps that would have prevented a known and preventable complication. 8. Delayed detection of patient deterioration. Readmitted because hospital failed to facilitate early detection and treatment of deterioration Each category suggests a general improvement tactic (See list two). • The distribution of readmissions among these categories is not well known • What percentage of readmissions is preventable? • How are preventable readmissions distributed among the eight categories? • Empirical investigation is needed to answer these questions (Strategy 1).
List Two: General Tactics for Reducing Preventable Readmissions 1.Clear readmission criteria. Develop and employ clear and consistent readmission criteria. Develop alternatives to readmission (such as rapid treatment centers, observation areas) 6. Education of family Develop and provide education to family on the post-discharge care of patients. Ensure that resources have been identified and provided. Ensure that appropriate assistance is available. 2. Clear discharge criteria Develop clear and consistent discharge criteria 7. Community services facilitation Identify the patient needs that can be met by community services and resources; identify the services and resources available in the community; match them up; facilitate appropriate contact, communication and coordination among community providers, PCPs and family. 3. HAC-prevention teams 4/5. Comprehensive post-discharge POC Assess potential complications prior to discharge and incorporate preventative measures into post-discharge plan of care. Identify patient’s post-discharge care requirements; identify needed care activities and resources; incorporate these into an effective post-discharge plan of care Actively involve patient’s PCP in post-discharge care 8. Facilitation of early problem detection Facilitate early detection of problems by the family and community physician. General activities include: clear communication with PCP, facilitation of appointment with PCP, and providing families with a clear and easy method for contacting clinical experts, and educating families on the identification of potential problems • To some extent these may be effective as general tactics (Strategy 2). But to be genuinely effective, they commonly need to be tailored to the patient, the diagnosis, the family, or the circumstances (Strategy 3). • Diagnosis-specific and risk-specific discharge criteria • Preventive actions (bundles) specific to each iatrogenic condition • Diagnosis-specific discharge planning • Patient-specific and risk-specific planning to minimize complications • Diagnosis-specific and family-specific education • Community-specific coordination of care • Diagnosis-specific and risk-specific problem-detection strategies • This task is aided considerably if investigative data on the distribution of causal categories and the distribution of diagnostic categories are available.
Strategy 1: Investigation • Conduct empirical investigation of readmissions: • Identify preventable readmissions • Classify by category • Classify by diagnosis • Develop databases • Strategy 2: General tactics • Employ general tactics where they are likely to be effective • Use them to structure specific preventive activities • Strategy 3: Specific preventive activities • Undertake specific preventive activities structured by general strategies and informed by investigative data • Diagnosis-specific and risk-specific discharge criteria • Preventive actions (bundles) specific to each iatrogenic condition • Diagnosis-specific discharge planning • Patient-specific and risk-specific planning to minimize complications • Diagnosis-specific and family-specific education • Community-specific coordination of care • Diagnosis-specific and risk-specific problem-detection strategies