Download
1 / 1

E N D
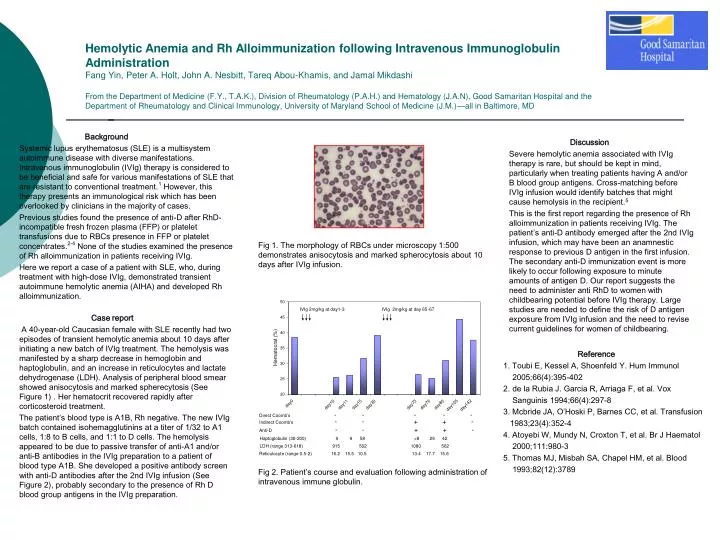
Hemolytic Anemia and Rh Alloimmunization following Intravenous Immunoglobulin AdministrationFang Yin, Peter A. Holt, John A. Nesbitt, Tareq Abou-Khamis, and Jamal MikdashiFrom the Department of Medicine (F.Y., T.A.K.), Division of Rheumatology (P.A.H.) and Hematology (J.A.N), Good Samaritan Hospital and the Department of Rheumatology and Clinical Immunology, University of Maryland School of Medicine (J.M.)—all in Baltimore, MD Background Systemic lupus erythematosus (SLE) is a multisystem autoimmune disease with diverse manifestations. Intravenous immunoglobulin (IVIg) therapy is considered to be beneficial and safe for various manifestations of SLE that are resistant to conventional treatment.1 However, this therapy presents an immunological risk which has been overlooked by clinicians in the majority of cases. Previous studies found the presence of anti-D after RhD-incompatible fresh frozen plasma (FFP) or platelet transfusions due to RBCs presence in FFP or platelet concentrates.2-4 None of the studies examined the presence of Rh alloimmunization in patients receiving IVIg. Here we report a case of a patient with SLE, who, during treatment with high-dose IVIg, demonstrated transient autoimmune hemolytic anemia (AIHA) and developed Rh alloimmunization. Case report A 40-year-old Caucasian female with SLE recently had two episodes of transient hemolytic anemia about 10 days after initiating a new batch of IVIg treatment. The hemolysis was manifested by a sharp decrease in hemoglobin and haptoglobulin, and an increase in reticulocytes and lactate dehydrogenase (LDH). Analysis of peripheral blood smear showed anisocytosis and marked spherecytosis (See Figure 1) . Her hematocrit recovered rapidly after corticosteroid treatment. The patient’s blood type is A1B, Rh negative. The new IVIg batch contained isohemagglutinins at a titer of 1/32 to A1 cells, 1:8 to B cells, and 1:1 to D cells. The hemolysis appeared to be due to passive transfer of anti-A1 and/or anti-B antibodies in the IVIg preparation to a patient of blood type A1B. She developed a positive antibody screen with anti-D antibodies after the 2nd IVIg infusion (See Figure 2), probably secondary to the presence of Rh D blood group antigens in the IVIg preparation. Reference 1. Toubi E, Kessel A, Shoenfeld Y. Hum Immunol 2005;66(4):395-402 2. de la Rubia J. Garcia R, Arriaga F, et al. Vox Sanguinis 1994;66(4):297-8 3. Mcbride JA, O’Hoski P, Barnes CC, et al. Transfusion 1983;23(4):352-4 4. Atoyebi W, Mundy N, Croxton T, et al. Br J Haematol 2000;111:980-3 5. Thomas MJ, Misbah SA, Chapel HM, et al. Blood 1993;82(12):3789 Discussion Severe hemolytic anemia associated with IVIg therapy is rare, but should be kept in mind, particularly when treating patients having A and/or B blood group antigens. Cross-matching before IVIg infusion would identify batches that might cause hemolysis in the recipient.5 This is the first report regarding the presence of Rh alloimmunization in patients receiving IVIg. The patient’s anti-D antibody emerged after the 2nd IVIg infusion, which may have been an anamnestic response to previous D antigen in the first infusion. The secondary anti-D immunization event is more likely to occur following exposure to minute amounts of antigen D. Our report suggests the need to administer anti RhD to women with childbearing potential before IVIg therapy. Large studies are needed to define the risk of D antigen exposure from IVIg infusion and the need to revise current guidelines for women of childbearing. Fig 1. The morphology of RBCs under microscopy 1:500 demonstrates anisocytosis and marked spherocytosis about 10 days after IVIg infusion. Fig 2. Patient’s course and evaluation following administration of intravenous immune globulin.






















