Download
1 / 26
260 likes | 342 Views
Affordable Care Act Implementation: Where We Stand at 3 Years. Molly Droge, MD, FAAP Chair, Access to Care Subcommittee to Committee on Federal Government Affairs April 29, 2013 AAP Legislative Conference Washington, D.C. AAP Staff, Title. Agenda Workshop I.

E N D
Affordable Care Act Implementation:Where We Stand at 3 Years Molly Droge, MD, FAAP Chair, Access to Care Subcommittee to Committee on Federal Government Affairs April 29, 2013 AAP Legislative ConferenceWashington, D.C. AAP Staff, Title
Agenda Workshop I 9:55 – 11:05 ACA Implementation 9:55- 10:00 Dr. McManus: Welcome & Introductions 10:00-10:20 Dr. Droge: “ACA Implementation: Where we Stand at 3 years” 10:20-10:40 Ms. Oakar: “Perspectives from HHS” 10:40- 10:50 Dr. McManus: “Experience with Massachusetts’ Exchange” 10:50-11:05 Discussion, Q&A
I have no relevant financial relationships with the manufacturer(s) of any commercial product(s) and/or provider of commercial services discussed in this CME activity Molly Droge, MD, FAAP
Patient Protection and Affordable Care Act (ACA) Signed Into Law on March 23, 2010 AAP Priorities for the ACA Coverage: Quality health insurance for all children Benefits: Affordable, age-appropriate benefits in a medical home Access: Payment rates and workforce support to provideaccess to covered services It’s 2013: How is ACA Implementation going?
What You Should Know About the ACA • ACA increases health insurance COVERAGE for 32 million uninsured children, families, and individuals by 2019 • It provides age-appropriate BENEFITS to children with Bright Futures Guidelines and Pediatric-specific Essential Health Benefits (EHBs) in new Exchanges • It improves ACCESS to covered services in multiple ways: • New marketplaces to compare and purchase insurance • Medicaid Expansion to 133% FPL • Tax credits to help small businesses purchase ESI for employees • Funding to expand Workforce, to build more Health care facilities, andto improve Medicaid Payment in 2013-2014
Coverage Expansion Framework • Individual mandate • Subsidies up to 400% of poverty line • Employer requirements – tax credits • Insurance market reforms • Insurance exchanges – help individuals and small business purchase insurance • Medicaid expansion – 133% of federal poverty line
Child Health Gains From ACA • More insurance options for children and families with Exchanges, Small business tax credits, Premium Assistance <400% FPL, and more • Children are more likely to be insured and to stay insured if parents are insured • Bright Futures as standard for ACA preventive care • Maintenance of Effort for Medicaid/CHIP programs • CHIP program in Arizona in 2010 • ACA Consumer Protection and Insurance Industry Reforms
ACA Consumer Protection Reforms • Prohibit: • pre-existing condition exclusions for children March 2010 (and for adults in 2014) • lifetime coverage limitsand restricted annual limits • cost sharing for preventive care • rescissions • Allow: • dependent care coverage to age 26 on parents’ insurance with consent (Results!) • choice of provider (primary care, OB/GYN, pediatrics) without a referral
ACA Insurance Industry Reforms • Temporary Pre-Existing Condition Insurance Plans from 2010 until 2014 • State Rate Review (+/-Approval) of Insurer Premium Increase Requests • Medical Loss Ratio (MLR) Requirements for Insurers => -Rebates to Consumers if Targets not met -Results! • New Insurance Exchanges
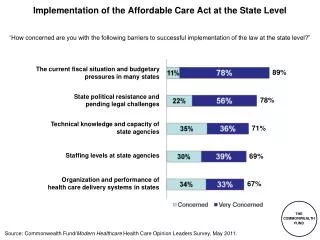
Key ACA Implementation Issues Health Insurance Exchanges • States’ choice of how to set up new Marketplace: • 18 States have declared intention to establish a state-based exchange • 7 states have planned for partnership, or hybrid state/federal exchanges • 26 states have defaulted to federal exchange • Tight Timeline in 2013 • Exchanges matter for exchange-based coverage, but also for links to Medicaid/CHIP enrollment
Key ACA Implementation IssuesEssential Health Benefits • EHB Final Rule gave states great flexibility to choose an already existing health plan as the state’s benchmark EHB package • If no choice by the state, default benchmark is largest small business plan in the state • AAP resource on deficiencies in employer-based insurance coverage • CHIP reauthorization as a vehicle for solution?
Key ACA Implementation Issues:Medicaid Expansion • ACA expands Medicaid eligibility to adults under 65 up to 133% FPL beginning in 2014 • Post-SCOTUS decision, states may decide whether to expand their program or not • Leaning toward not expanding: 10 states • Leaning toward expanding: 8 states • Expanding: 18 states (includes DC) • Undecided: 15 states
What Happens if State Chooses Not to Expand Medicaid in 2014? • Miss opportunity to finance Medicaid up to 133% with federal dollars • 100% federal dollars 2014-2016 • Gradually decreases to 90% federal match by 2020 and beyond • Send citizens’ federal tax dollars to other states • Miss opportunity to create thousands of jobs in the state • Continue “hidden health care tax” for citizens and businesses • ACA mandates reduced federal disproportionate share payments to hospitals after Medicaid Expansion in 2014 • Delaying decision to Expand Medicaid until next year guarantees loss of portion of federal funds
“Family Glitch” Medicaid Expansion
Key Issues for Children in Eligibility Rules • Affordability Standard for ESI Family Coverage (“Family Glitch”) • Alignment of Medicaid/CHIP/Exchange Eligibility Standards • Requirement to Enroll Children Before Parents • Custodial Parents Claim on Child as Dependent • Language Access Mandate for LEP Individuals • CMS Support for Waivers and 12 month Continuous Eligibility Beyond Children
ACA’s Impact Varies Based on Key Policy Decisions Number and Characteristics of Uninsured Children Under Baseline and Different Scenarios Source: Kenney, Genevieve, et al., Improving Coverage For Children Under Health Reform Will Require Maintaining Current Eligibility Standards For Medicaid And CHIP, Health Affairs Vol. 30, No. 12 (December, 2011), 2371-2381. * The estimates provided for CHIP Lapse and MOE Repeal range depending on assumptions about high or low ESI and Exchange takeup rates – the value assigned here is an average.
Benefit Needs for Healthy Children • Children are not small adults • Most pediatric care is preventive and most children are healthy • After coverage, appropriate pediatric benefits is the most important concern for pediatricians • Overarching concern for healthy children is insurance coverage with age-appropriate benefits that will address their unique needs
Benefit Needs for CYSHCN • Children and Youth with Special Health Care Needs (CYSHCN) • 1 in 5 U.S households with children has at least one Child or Youth with Special Health Care Needs (8.8 million U. S. households) • Many are heavily dependent on Medicaid to “fill in the gaps” of private insurance; • about 60% of CYSHCN depend on private insurance only • but families have high out of pocket costs • Overarching concern for families with CYSCHN is adequacy of insurance and avoiding medical bankruptcy
ACA Benefits for Children • Bright Futures services for no copay for new plans • Essential Health Benefits: pediatric services including oral and vision • HHS Rules allow State flexibility in substituting within EHB categories • If a child does get sick, ACA mandates no pre-existing conditions exclusions, no annual or lifetime limits, and no rescissions • Out of pocket maximums per year pegged to health savings account level ($5,950/individual, $11,900/family) • Challenges
ACA Benefits for Pediatricians • Pediatricians practice in a variety of settings in challenging economic times • Small practices consolidating into larger practices • HIGH overhead costs requires using private pay patients to balance out inadequate public program payment, or no payments from care of uninsured patients • Concern for pediatricians is financial viability of pediatric practices and professional needs of Advocacy at both State Chapter level and Federal Level
ACA Benefits for Pediatricians • Medicaid payment increase to 100% of Medicare rates for 2013-2014 for E&M codes • Small business tax credits for small pediatric practices to defray employees’ insurance cost • Workforce loan forgiveness authorizations for primary care (NHSC) and pediatric subspecialty (PHSA sec. 775) • All embedded in the ACA with the intense advocacy efforts of AAP leadership and members
Key ACA Implementation Issues:Medicaid Payment Increase Regulations • Increases Medicaid payment for E/M Codes to 100% of Medicare in 2013/2014 or June 2009 (whichever is higher) (win!) • Includes Pediatric medical and surgical subspecialists (win!) • Applies to Managed Care, employed physicians (win!) • Increases Immunization Rate payment for Medicaid/VFC to new Maximum Regional Charge or 90460 in Medicare (whichever is lower) • Lasts only 2 years… need to prove effectiveness of increasing participation in Medicaid to reauthorize, or it becomes our “SGR”
ACA Implementation Timeline - Major Policies • New Consumer Protections for children (and adults in 2014) • Preventive Care Without Cost-Sharing • Temporary Pre-existing Condition Insurance Plans • Dependent Coverage up to age 26 • Maintenance of Effort (MOE) in Medicaid • Rebuild Primary Care Workforce • Medicare ”Donut Hole” Prescription Drug Assistance • Small Business Tax Credits • Prevention and Public Health Fund • Premium Rate Review by States • Strengthening Community Health Centers 2010 • Prescription Drug Discounts • Free Preventive Care for Seniors • New Center for Medicare/Medicaid Innovation for Quality and Efficiency • Medical Loss Ratio for Insurers • Address Overpayments to Big Insurers in Medicare Advantage • Community Care Transitions Programs • Extend Medicare Trust Fund with innovations to bring down costs 2011
ACA Implementation Timeline - Major Policies • Accountable Care Organizations (Integrated health systems with risk/rewards sharing) • Health Information Technology improvements to reduce paperwork and administrative costs • Understand and addresshealth disparities • Value-Based Purchasing programs for hospitals to improve quality of care • 2012 • Increased Medicaid payments to Primary Care Doctors to 100% of Medicare Payments for E & M preventive care & Immunization Administration codes for 2013-2014 • Provides additional funding (FMAP) for CHIP through 2015 • Improve Preventive Health Coverage for adults in Medicaid at little or no costs • Expand authority to bundle payments • 2013
ACA Implementation Timeline - Major Policies • Insurance Exchanges • Expand Medicaid to 133% FPL • New Consumer Protections Reforms effective for Adults • Prohibit Pre-existing Conditions or Gender Discrimination for Adults • Eliminate Annual Limits on Insurance Coverage • Tax credits for incomes between 100%-400% FPL • Increase Small Business Tax Credit up to 50% of employer’s contribution • Young adults who are Foster Care alums can stay on Medicaid to age 26 years • Establish Individual Mandate/ Responsibility to have minimum health insurance coverage • 2014 • Penalty for failure to comply with individual mandate phased in by 2015 • 2015 • Option for state waivers to design alternative coverage programs • (Arkansas, 2013) • 2017 • Complete coverage of additional 32 million previously uninsured Americans through Exchanges • 2019