Download
1 / 27
270 likes | 465 Views
Understanding the Physician’s Role in Partnering for PDPM Success. Kendra Coco MPT, NHA, RAC-CT, RAC-CTA Director of Clinical Reimbursement 9/3/2019. Patient Driven Payment Model (PDPM). Effective October 1, 2019

E N D
Understanding the Physician’s Role in Partnering for PDPM Success Kendra Coco MPT, NHA, RAC-CT, RAC-CTA Director of Clinical Reimbursement 9/3/2019
Patient Driven Payment Model (PDPM) Effective October 1, 2019 Medicare A payment model that shifts focus from therapy utilization to patient characteristics Incentivizing SNFs to take on higher acuity patients with more complex conditions and comorbidities Payment is captured through MDS coding • Must have documentation support
Constant per diem rate • Variable per diem adjustment
Model Snapshot Higher needs = Higher Case Mix for each component Patient driven and holistic care model based on patient’s unique needs
Focus #1: Timeliness of Visits Admission - Visit goal within 24-48 hours • Provider documentation assists in obtaining & authenticating patient information, including medical diagnoses for initial MDS assessment • Initial MDS assessment due no later than day 8 however, • Some hospital interventions may be considered • Ie. IV fluids in 7 day look back Change of condition - Optional Interim Payment Assessment (IPA) • Can be completed if increased acuity & financial gain achieved
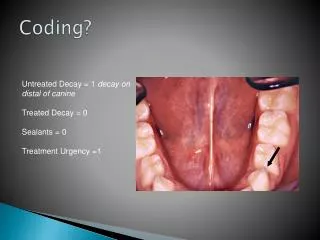
Focus #2: Diagnosis Accuracy Reason for SNF Admission • Influences all 5 Clinical Components PT, OT, SLP, Nursing, NTA • NTA diagnoses are paid 3x NTA Component rate for first 3 days Hospital assigned diagnoses may not be relevant or accurate • Acute illness & infections may be resolved • Red flags for audits Must be coded on initial MDS assessment & have documentation support
ICD-10 CM coding accuracy for PDPM Medical Diagnosis • Reason for the SNF stay (primary medical diagnosis) • Pertinent active Comorbidities • Highest degree of specificity Paints a detailed picture of the residents, conditions, areas of risk of exacerbation, comorbidity risks & prognosis Treatment Diagnosis • Relates to Medical Diagnoses • Related to assessment findings (standardized tests and measures) • Relates to goals & treatment plans • Highest degree of specificity
MDS Coding of Active Diagnoses Condition must be documented by MD, NP, PA, or CNS in the last 60 days • Direct relationship to current status • Functional • Cognitive • Mood • Behavioral • Medical treatments • Nurse monitoring • Risk of death **(except UTI-last 30 days) Past 7 days
RTP examples • Muscle weakness (generalized) • Age related osteoporosis without current pathological fracture • Fractures “unspecified” • Dyspnea, unspecified • Shortness of breath • Nausea, vomiting • Acute duodenal ulcer with hemorrhage Primary Diagnosis: RTP Diagnosis listed Return to Provider are considered not appropriate as primary diagnosis for a SNF stay Can report as secondary diagnosis on MDS and claim • Provider Query
CMS Mapping Tool “Return to Provider” Codes • Unspecified codes • Codes that don’t support inpatient SNF care Nearly 43% of eligible ICD-10 codes are RTP
Fracture Coding for PDPM Fractures coded (not aftercare) when surgeries repair the fracture • ORIF • Joint replacement Need to code as specific as possible • Open or closed otherwise defaults to closed • Displaced or nondisplaced defaults to displaced • Traumatic or pathological
Diagnosis influencing Non-Therapy Ancillaries (NTA) NTA Qualifiers Clinical Resources & supplies needed to care for resident Excludes therapy services Most common items: • Medications • Medical supplies • Labs • Respiratory Therapy Why? RUG IV did not take into consideration • Care • Points • $
Behaviors Impacting Nursing Component Hallucinations Delusions Behaviors Rejection of Care Wandering • Must have documentation support during MDS lookback • If no documentation, cannot code! • IDT review for rejection of care accuracy • Rejection of care includes: refusing showers, ADL assist, medications, treatments, labs, assessments, etc.
Health Conditions Impacting Nursing & NTA Component Shortness of Breath/Trouble Breathing Lying Flat Fever Vomiting Ostomy and Intermittent Catheterization Urinary Toileting and/or Bowel Toileting Program
Surgical Procedure Impacting the Therapy Components Impacts all 3 Components Major surgical procedure: • At least 1 inpatient day within an acute care hospital within the last 30 days prior to SNF admission • Carried some degree of risk to patient’s life or potential disability
Swallowing/Nutritional Status Signs & symptoms of possible swallowing disorder impacting ST component • Loss of liquids/solids when eating/drinking • Holding food in mouth/cheeks or residual food in mouth after meals • Coughing or choking during meals or swallowing meds • Complaints of difficulty or pain with swallowing Mechanically Altered Diet while a resident Impacting the Nursing & NTA components Significant Weight Loss Impact Nursing Component IV Feeding & Tube feeding impact Nursing & NTA Component
Skin Conditions Impacting Nursing & NTA Components Pressure relieving chair and/or bed Turning/repositioning Nutrition or hydration intervention Pressure ulcer care Application of non-surgical dressings (not feet) Application of ointments (not feet) Current Unhealed pressure ulcers Venous/Arterial Ulcers Foot Infection Diabetic Foot Ulcer, or Other open lesion on foot Open Lesions, Surgical Wounds 2 or more Skin and Ulcer/Injury Treatments
Medications impacting the Nursing Component Insulin Injections and insulin order changes
Special Treatments, Procedures, & Programs While a Resident impacting the Nursing, NTA & SLP Components Chemotherapy Radiation Respiratory & Oxygen Therapy Suctioning Tracheostomy Care Invasive Mechanical Ventilator IV Medication Transfusion Dialysis Isolation Restorative Programs
Focus #3: Managing Medically Complex Patients Prevent unnecessary use of resources, including avoidable rehospitalizations Advance Care Planning Change of Condition • May qualify for IPA (Interim Payment Assessment) • Reset payment if resident characteristics change
Focus #4: Pharmacy cost containment Pharmacy cost is reimbursed under NTA category • Consider pharmacy formulary • Medicare does not distinguish between branded & generic medications • IV infusions bring higher reimbursement, but branded IV meds may cost more than the entire NTA allowance • Antibiotic stewardship is equally important for patient safety & cost reduction
Focus #5: Therapy Service Collaboration Therapy no longer a driver for SNF reimbursement but still needed for outcomes Patient qualifies for a PT, OT, ST Component whether or not therapy is ordered • Reductions risk audits - PEPPER report • Top of License • Restorative Nursing collaboration with therapy Provider should continue to be closely involved in initiation, care planning, and cessation of therapy services to streamline & safeguard efficiency & integrity
Kendra Coco MPT, NHA, RAC-CT, RAC-CTA Director of Clinical Reimbursement