Download
1 / 43
430 likes | 930 Views
Basics of Transfusion Therapy. Resident Education Lecture Series. Hemoglobin Level and Symptoms. HGB (GM%) SYMPTOMS 9-11 MINIMAL 7.5 EXERTIONAL DYSPNEA 6.0 WEAKNESS 3.0 DYSPNEA AT REST 2-2.5 HEART FAILURE. LINMAN NEJM 279:812, 1968. RBC Transfusion: Indications.

E N D
Basics of Transfusion Therapy Resident Education Lecture Series
Hemoglobin Level and Symptoms HGB (GM%)SYMPTOMS 9-11 MINIMAL 7.5 EXERTIONAL DYSPNEA 6.0 WEAKNESS 3.0 DYSPNEA AT REST 2-2.5 HEART FAILURE LINMAN NEJM 279:812, 1968
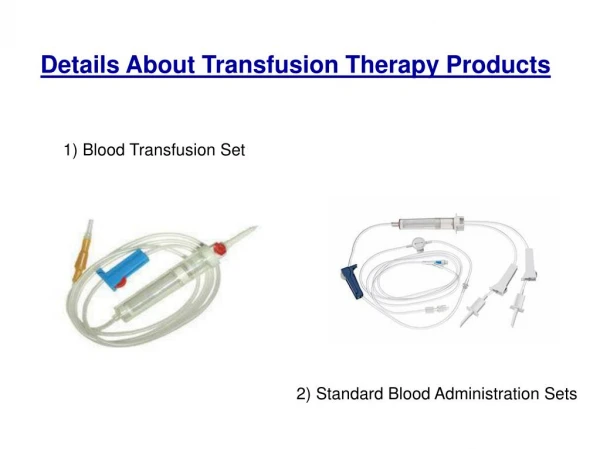
RBC Transfusion: Indications • Acute Blood Loss • Symptomatic Anemia • Suboptimal O2 Capacity • Exchange (SS, Co)
RBC Transfusion: The Bathtub Principle Kidney Kidney Kidney 100 30 0 100 30 0 100 40 0 Blood Volume Blood Volume Blood Volume
Pre-Transfusion Testing • BLOOD TYPING: • ABO, D Antigens only (Other antigens are weak immunogens) • ANTIBODY SCREEN: • Patient serum vs. cell panel • CROSSMATCH • Major: Patient Serum vs. Donor Cells
RBC Products • PRBCMOST TRANSFUSIONS • WHOLE BLOOD ACUTE BLEEDING EXCHANGE PLASMA NEEDED • WASHED REMOVE PLASMA • FROZEN RARE RBC PHENOTYPE • IRRADIATED IMMUNODEFICIENT • CMV NEGATIVE IMMUNODEFICIENT SERONEGATIVE, NEONATE
RBC Transfusion Volume • Usual: Up to 15cc/Kg in 3-4 hours • Unusual: Acute Hemorrhage: replace ongoing losses Chronic Anemia, Heart Failure, îBP 2cc/Kg/Gm HGB Diuretic Exchange
Transfusion Volume • 10cc/Kg PRBC 2.4 GM% in HGB 10cc/kg = X cc/kg 2.4 GM% Desired HGB rise • PRBC cc = Blood Volume x (HGBF- HGBI) HGBT BV=70cc/KG, 80-90cc/KG newborn
Hemolytic Transfusion Reactions • Acute HTR 1/25,000 • Fatal Acute HTR 1-4/1,000,000 • Delayed HTR 1/5-10,000
Symptoms and Signs of Acute Hemolytic Reactions • Severe Back Pain • Substernal Tightness, Dyspnea • Hypotension / Circulatory collapse • Vomiting, diarrhea • Icterus • Hemoglobinuria • Renal shutdown • Diffuse Oozing from wounds/punctures
Response to Suspected Hemolytic Reaction • Stop Transfusion • Hydrate • Specimens to Blood Bank • Unit/Bag • Serum • Red cells • Urine
Acute Hemolysis: Diagnosis • Do a direct antiglobulin test on post-transfusion sample • Obtain post-transfusion blood and urine and inspect visually • Recheck paperwork • Recheck ABO type of unit and pre-and post-transfusion specimens • Run urinalysis - to check for hemoglobinuria
Cause of Acute HTR • ABO incompatibility:source of error • 10% at phlebotomy/labeling • 23% in Transfusion Lab • 67% transfusion administration (at the bedside)
Leukocyte Associated FNHTR Transfusion GVHD Neonatal Neutropenia Immunoglobulin Associated Urticaria/Fever Ig E TRALI Platelet Associated Post transfusion Purpura Neonatal Thrombocytopenia Metabolic/ Physical Citrate Toxicity Hypothermia Circulatory Overload Massive Transfusions Haemostatic Abnormalities Metabolic complications Hgb-O2 Curve Shift Nonhemolytic Transfusion Reactions
Risk of Transfusion-Transmitted Infection HIV 1 in 2,000,000 Hepatitis C 1 in 2,000,000 Hepatitis B 1 in 175,000 Hepatitis A Rare HTLV I/II 1 in 3,000,000 Bacteria 1/3,000 (for platelets) Malaria, T Cruzi, Babesia, Yersinia, Syphilis, Lyme, CJD, West Nile Virus…??
Post Transfusion HCV PercentNumber Incidence 5-10 150-300,000 Chronic 50 75-150,000 Cirrhosis 20 15-30,000
Neonatal Post Transfusion CMV • Incidence: 25% of seronegative infants receiving >50ml CMV seropositive blood • Severity 50% severe or lethal manifestations
Neonatal Transfusion CMV Prevention by Filtering Blood Seroconvert/Total Filtered PRBC: 0/30 Unfiltered PRBC: 9/42 Gilbert, L1:98:228, 1989
Prevention of Post Transfusion Infection • Don’t Transfuse • Minimize Transfusion • Limited Donors (dedicated units) • Autologous Transfusions • Erythropoetin • Donor Screening: HIV Ab, HIV NAT, HCV Ab, HCV NAT, HBV Ag, Ab, HBc Ab, VDRL, West Nile NAT, HTLVI/II Ab, CMV Ab, Bacterial Culture (Platelets)
Strategies to Decrease Operative RBC Transfusion Hemostasis Hemodilution Cell salvage DDAVP Autologous Transfusion Erythropoetin
Relapse Remission 100 100-500 500-1000 1000 Neutropenia: infection risk Bodey. Ann Int Med 64:328, 1966.
WBC Indications 2004 • PMN: Newborn Sepsis Congenital/Acquired Neutropenia PMN Dysfunction Refractory Gram Negative Sepsis • Ly: Disseminated Varicella-Zoster
WBC transfusion:Logistics • Donors Receive G-CSF +/- Decadron • 2-3 Hour Cytapheresis • 1010 Cells by Standards • Donors pretested for ID markers • Cells decay rapidly: limited value at > 6 hours post-collection • Quantitative impact limited
Fresh Frozen Plasma • 200-250 ml of plasma containing all clotting factors, AT III, Protein C & S. • Compatibility Important • Can Give: A plasma to A or O patient B plasma to B or O patient O plasma to O patient AB plasma to anyone
Indications: FFP • Replacement of Coagulation Factors • Abnormal Bleeding with coagulopathy • Multiple factor deficiency: • Liver disease • DIC • Reversal of Warfarin • Dilutional • Isolated factor deficiency-no concentrate • Factor XI, XIII • Replacement of regulatory proteins • TTP, Hereditary angioedema • Not indicated for: volume expansion, reversal of Heparin, correction of INR < 1.5
Guidelines: FFP Use • Usual dosing: Adult 10ml/Kg Peds 10-15ml/Kg • 15-20% rise in factor levels • Usually does not correct laboratory coagulation status to “normal”
Cryoprecipitate • 10-15 ml per unit (bag) • Fibrinogen 250 mg • Factor VIII 80-120 units • Von Willebrand Factor 40-70% of FFP • Factor XIII 20-30% of FFP • Fibronectin 20-40 mg
Cryoprecipitate: Dosing • 1-2 Units / 10 Kg • Expect 60-100 mg/dl rise in fibrinogen • Goal: Fibrinogen 70-100 mg/dl
Platelets: Risk of Spontaneous Hemorrhage CountSite > 40,000 Minimal 20-40,000 GI Mucosa 5-20 Skin, Mucus Membranes < 5 CNS, Lung
Uremia vWD 40 WAS 30 AA ASA Bleeding time (min) 20 ITP 10 0 0 50 100 150 200 250 300 Platelets (/microL) Harker. NEJM 287:155, 1972.
Prophylactic Platelet TX Guidelines Platelet Count/μlRecommendation 0-5,000 Always 5-10,000 If Febrile of Minor Bleeding 11-20,000 If coagulopathy or minor procedure >20,000 If Major Bleed or invasive procedure
Transfused Platelets/Survival • 6 units = 1 single donor unit (SDP); available as ¼, ½ and full SDP • Dose: child 1 unit/5-6 kg adult 1 unit/8-10 kg • Lifespan: 7-10 Days Native 2-3 Days Transfused • Factors shortening Lifespan: • Fever, Sepsis • HLA, Platelet Specific Abs • DIC • Product Age?
From ABP Certifying Exam Content Outline • 2. Transfusion and collection of blood • Understand the risk of transmitting infectious diseases during blood transfusion(s) • Recognize that erythrocyte transfusions may be associated with hemolytic, febrile, and urticarial reactions • Understand the role of erythrocyte transfusions in the management of anemia
Credits • Bruce Camitta MDM W Lankiewicz MD