Download
1 / 53
530 likes | 800 Views
Why A New Change in Strategy Should be Considered for Medical Oncology Coding and Reimbursement Planning for the Future of “Value Based Purchasing” MOASC December 1, 2005. “We Bring The Pieces Together For You”. NBC. Neltner Billing & Consulting Services, Inc. 6463 Taylor Mill Road

E N D
Why A New Change in Strategy Should be Considered for Medical Oncology Coding and Reimbursement Planning for the Future of “Value Based Purchasing” MOASC December 1, 2005 Neltner Billing & Consulting Services “We Bring The Pieces Together For You”
NBC • Neltner Billing & Consulting Services, Inc. 6463 Taylor Mill Road Independence, KY 41051 (800) 676-7639 (859) 363-4900 www.neltnerbilling.com • Martin E Neltner, President (859) 363-4981 office (859) 743-6192 cell mneltner@earthlink.net Neltner Billing & Consulting Services
Expertise • 25 years working in oncology • Began the AWP process for payment of drugs 1984 • Assisted in founding several state oncology societies 1986-1992 • Authored Oncology Services Manual(s) used for coding of oncology services 1989-1995 • Coding for start-stop • ALJ wins – 650 wins for appropriate coding of reservoir maintenance • Two proposals to AMA for new coding Neltner Billing & Consulting Services
APOLLO 13 (1995) Houston we've got a problem. • Failure is Not an Option there fore We must • Practice the OZ Principle Conners, Smith, Hickman • Accountability and Responsibility • Built to Last --Collins, Forras • Execution The Discipline of Getting Things Done-- Bossidy, Charan, • Healing our Health Care System, Abramsom • Saving Lives and Saving Money, Newt Gingrich • Transformation of Health and Health Care Neltner Billing & Consulting Services
Who Moved the Oncology Cheese? • Snuff and Scurry • Hem • Haw Neltner Billing & Consulting Services
Oncology is not • Simple Medicine • Routine • Drugs and such • Putting patients in the grave while the IV is dripping • All about me and not the patient Neltner Billing & Consulting Services
Why does Oncology • Appear Simple • Routine because I do this every day and I don’t want to charge a higher visit • Have a problem getting injection drugs paid • Have this love hate relationship with the Congress • Is this a myth or reality • Have a problem obtaining excellent coding with the AMA ? Neltner Billing & Consulting Services
So what is the problem • Making our argument about seeking appropriate reimbursement • Creating new Cpt codes that make sense and are simple to use • Arguing for treatment planning and ongoing management codes • Getting paid for our cost Neltner Billing & Consulting Services
More Patients The Wild Bunch Generation • By 2030, there will be about 70 million older persons, more than twice their number in 2000 -- source “ Profile of Older Americans study by the Council on aging • What is happening to this population now? • More cancers in age bracket 45 – 60 Neltner Billing & Consulting Services
1996 Article in Courier Journal Louisville Kentucky • Edition=MET:METRO_7_STAR; Date=11/09/1996; Section=NEWS; Page=01A; • -------------------------------- • Headline: Cancer drug's cost shows how hospitals vary wildly on pricing • SubHead: IT PAYS TO SHOP FOR THE BEST PRICE • Byline: DICK KAUKAS, The Courier-Journal • Cancer patients can pay from $224 to $696 per vial of Taxol at different hospitals, which buy the drug for $146 vial. Neltner Billing & Consulting Services
Chamber of CommerceJuly 17, 2003 Cost and Quality Impact of Drug Company Marketing to Physicians • July 17, 2003 • Cost and Quality Impact of Drug Company Marketing to Physicians • Earlier this month, the Blue Cross and Blue Shield Association (BCBSA) released the report -- "Getting Doctors to Say 'Yes' to Drugs: the Cost and Quality Impact of Drug Company Marketing to Physicians" -- examining the extent to which pharmaceutical companies' promotional efforts contribute to both the appropriate and inappropriate use of medications and their impact on the quality and cost of patient care.According to the report, pharmaceutical companies spend billions of dollars to influence which medications physicians prescribe and the duration of the treatment. While many drugs are extraordinarily beneficial, it does not discount the need to explore the economic effects of industry marketing. A balanced assessment of the "value of medicines" should look at both sides of the equation. Neltner Billing & Consulting Services
Coverage • National coverage • National coverage article (NCA) • National coverage determination (NCD) • Determines if an item or service is covered • Does not assign a code or payment • Local coverage • Local medical review policy (LMRP) • Local coverage determination (LCD) • Beneficiaries • Have the right to challenge NCD/LCDs Neltner Billing & Consulting Services
Agenda • The History • Short lesson in the history of oncology coding • Why is history critical for the New Opportunity? Neltner Billing & Consulting Services
History • Prior to 1984 (before CPT) Medicare had an RVU-based payment system • CPT codes changed everything – UCR payment methodology for 5 years • Prior to 1986 Oncology billed using 96500 series codes • Three push codes • Four infusion codes • Supplies were recognized and paid • Professional treatment planning was recognized with the 60/40% rule • Prior to 1989 Medicare continued to recognize treatment planning • $90 allowable for modifier -26 changed to Y1000 (OH) and X5050 (IN) • $150 allowable for 96410 only in certain states • Drugs paid at AWP+20% • Except in KY and OH where drugs were paid at AWP Neltner Billing & Consulting Services
A Series of Missed Opportunities • Harvard study – missed opportunity • Inherent reasonableness and gap-filled • Conversion of data in 1989 • CMS used historical data not cost data • $40 – 96410 • $18 – 96412 • CMS questioned validity of cost data supplied by oncology community • No professional costs requested or recognized • Transition period – missed opportunity • RVUs implemented in 1994 • RVUs converted to resource-based in 1997 • Oncology survey data was not submitted until 2003 and accepted in 2004 • Now we have a RESOURCE-BASED PAYMENT SYSTEM • RUC AND AMA PROCESS Neltner Billing & Consulting Services
Historical Drug Payment Policy • Medicare rule has always been to pay cost • 1984 Medicare declared AWP Drug Topics Redbook monthly update would be used to define cost of drugs • Tennessee attempted to impose payment of drugs at invoice +5% in 1995 • 1989 drug policy changed with RBRVS • The real missed opportunity • ASCO agreed no professional fee in oncology codes in exchange for keeping drugs at AWP +++ Neltner Billing & Consulting Services
Historical Technical Precedent • 96500 or 96400 series codes did not describe cognitive work of physician • 96500 or 96400 series codes were “technical” only • 19 codes – only 4 were used • “Needle In, Needle Out” vs “Start/Stop” • Pro fee would be recognized in E&M codes • 1995/1997 AMA E&M documentation guidelines introduced – missed opportunity Neltner Billing & Consulting Services
Historical Professional Recognition • Twice we requested the AMA to revise the oncology codes to reintroduce treatment planning • 1995 NBC, Ohio/West Virginia and MOASC • Told by the AMA panel to use prolonged services and level five visits for treatment planning • 2003 NBC and MOASC • Submitted request to AMA for new codes 10/03 • Oncology community would not support • 12/03 MMA law passed requiring CMS to “promptly evaluate” • 2005 Congress mandate resulted in G codes Neltner Billing & Consulting Services
Oncology E&M Utilization 89–98 Neltner Billing & Consulting Services
Oncology E&M Utilization 00-05 Neltner Billing & Consulting Services
AMA News January 2005Medicare zeroes in on E&M coding as key source of payment mistakes • But nearly $1 billion stayed in the federal coffers when it should have gone to medical professionals, and the agency suspects that the same coding confusion could be largely to blame. A special investigation of underpayments found that the vast majority of the reimbursement shortfalls to physicians alone could be linked to a familiar administrative headache: the evaluation and management code. Studies from past years had focused only on overpayments. Neltner Billing & Consulting Services
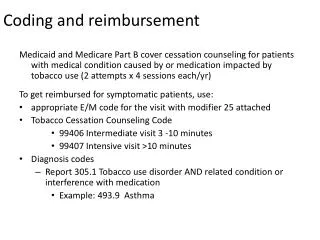
E&M Coding • Why oncologists did not bill higher visits • Fear of audits • Patients would have to pay higher co-pays • Oncologists and nurses felt $120 for 40 minutes of work was too expensive for patients Neltner Billing & Consulting Services
How can I make an argument for treatment planning ? • When down coding is occurring • This is routine to me • There is no story in the note to convey high complexity • I only bill a level V if I begin a new treatment Neltner Billing & Consulting Services
Fee Schedules • Two fee schedules are permitted • The high charge is not the payment • The Blues story in Indiana – high charge backfired • The high charge of the drug is a target for accusing the oncology community of abusing the patient and/or system • It is ironic that no one (in the oncology community) questions high payments for drugs yet we are so concerned about the high price of a level five visit Neltner Billing & Consulting Services
Whistle Blowers and Oncology • House Hearings • Congress heard testimony about the Florida case • Doctors were the bad guys • Now they are back in California • Medicaid case • New York and other states going after drug companies • Will the oncology community be next ? Neltner Billing & Consulting Services
AWP Crusade • Empire State Joins AWP Crusade • (Medical Newswire) New York Attorney General Eliot Spitzer joined a half dozen other states in suing drug makers over one of the hottest compliance hot buttons of recent years – alleged meddling with the average wholesale price that governs Medicare and Medicaid reimbursement. • In lawsuits filed Feb. 13, Spitzer accused GlaxoSmithKline and Pharmacia of reporting an inflated AWP and using the difference between the reported price and the amount it actually charged doctors, pharmacists and other health care providers – the so-called “spread” – to induce practitioners to prescribe their drugs. Providers make out well under the practice, since they obtain the drugs relatively cheaply, and get reimbursed for them at the significantly higher, AWP-pegged price. • Spitzer is expected to file a similar suit against Aventis in the near future. • A number of other states have filed similar lawsuits, including Nevada, Montana and California. The twist in the New York action, Spitzer says, is that the suits go after the drug companies with counts of commercial bribery and making false statements to government health plans, as well as consumer fraud. • State AGs aren’t the only ones fed up with the AWP system. The HHS Office of Inspector General has long bemoaned the fact that AWP pricing is out of step with actual acquisition costs, the General Accounting Office has raised concerns with the issue and Congress has worried over the matter – without, however, changing the statute that helps perpetuate the system. Neltner Billing & Consulting Services
Agenda • The Problems • Where is the oncology complexity? • Who “moved the cheese” in oncology reimbursement? • The continued erosion of oncology coding • 96530, BMB/BMA, G-codes • Why the AMA is a disappointment to solving the oncology coding problem • Failure of the NCCI edits • Why Congress and CMS don’t believe our story on payment for resources? • Why the demonstration project has backfired? Neltner Billing & Consulting Services
Where is Oncology Complexity? • Everything okay, give chemo • HPI, ROS, Exam • I don’t have time to document! • Where is the story? • 20 E&M audit wins in the past ten years is the testimony of why the story is important • Auditors are not oncology-trained • Auditors believe a change must occur in order to bill a level five visit Neltner Billing & Consulting Services
Who Moved My Cheese?(by Dr. Spencer Johnson) • NBC won audits for billing level fives • What does face-to-face mean? • NBC won an audit for billing prolonged services • NBC won over 750 audits for billing 96530 • Too bad the oncology community did not join in this effort • The wins would have been in the hundreds of thousands • Codes and payment policies may have been different in ‘05 Neltner Billing & Consulting Services
Reservoir Access and Maintenance • Formerly CPT code 96530 • AMA coding panel in August 2004 changed meaning of code without due process • 2005 coding panel did not give us a G-code for reservoir access during the episode of the chemo event • Panel said the oncology community was not using this code • Payment for G0363 bundled • Infusions and pushes • Injections – why? • Office visits – why? Neltner Billing & Consulting Services
Bone Marrow Procedures • Change in code due to lobby efforts • RVUs modified • NCCI and Dr. Rosen • The debate (we almost won) • Key destruction of practice expense value • Key destruction of professional work value • Stopped CMS once but apathy persisted • No action by ??? resulted in add-on G-code that drastically reduced practice expense and pro fee • No transparency in the CCI process • Why this has an impact on oncology reimbursement • Where is the oncology complexity? Neltner Billing & Consulting Services
96400 Injections • Another missed opportunity • CMS-1372-FC • Accepted ASCO practice expense survey data • Added physician work RVUs to drug administration procedures • Moved procedures out of zero-physician work pool • Increased allowable an additional 32% temporarily • 96400 allowable increased from $37.52 to $64.07 Neltner Billing & Consulting Services
Time and Motion of a G code • Service Time (Minutes) Practice Expenses • HCPCS Pre Intra Post Total Rate/Min Labor Supplies Equipment Total PE Payment • G0359 6 86 6 98 $ 0.79 $ 77.42 $ 22.77 $ 1.21 $ 101.40 $ 158.79 Neltner Billing & Consulting Services
Administrative Law Judges • Over whelming recognized separate payment for 96530 for 2004 claims • Also recognized level fives and prolonged services • Oncology community needs to fight for payment for this procedure • AMA & CMS need to be convinced once again Oncology was dealt a bad card • They will listen if oncology community fights for payment of resources Neltner Billing & Consulting Services
Demonstration Project • September 8th OIG preliminary assessment • Reported to Senate Finance Committee • Assessments not administered uniformly • Assessments do not collect data on interventions • Assessments “already part of the routine care” • Patient liability of almost $50M annually Neltner Billing & Consulting Services
Demonstration Project • Why the demonstration project is a failure • It’s just plain stupid • We fell into the trap • Take the money and run • Forget about quality • Forget about integrity • Do we have a treatment planning code? Neltner Billing & Consulting Services
Where is Oncology Complexity? • How can we ask for Oncology treatment planning codes when we are not billing lots of: • Level fives • Prolonged services • Higher visits for injections Neltner Billing & Consulting Services
The Nurse Assessment Visit Should every patient be evaluated ? What is the physician work and expense to provide service? Are these allowables correct? How many bill an injection vs visit How many bill a higher visit on the day of injection What does the LMRP or LCD say ???? Pro fee practice expense Nurse visit 99211 $6.44 $15.159 Injection G0351 $6.44 $12.13 Neltner Billing & Consulting Services
Pursuit of Purpose • What is our purpose? • What is our mission statement? • Oncology community must be engaged in the fight to prove its complexity by telling a story in the note that we are doing a great job to contain cost of care while providing excellent care Neltner Billing & Consulting Services
Prove Oncology Complexity • “It doesn’t happen until it happens” • Prolonged is Oncology opportunity • Level fives is Oncology opportunity • Level iii, iv are correct codes for injections of red and white cell patients Neltner Billing & Consulting Services
Historical Perspective • Why is the historical perspective necessary for the New Opportunity? • We missed many opportunities in the past • In 2006: • CPT codes will be deleted • G-codes will be converted to CPT codes • AMA is defining codes according to Medicare payment policies • Do drug administration codes capture our resources? • What additional codes are needed and how can we get them recognized? • Payers are looking at new drug reimbursement methodologies • CAP • ASP Neltner Billing & Consulting Services
Oncology Solutions • Must be willing to step up to the plate • We continue to be the solution for cost-effective care • Embrace the strategy that the Oncology community is willing to be a partner to help CMS and other insurance companies purchase drugs at the lowest cost. • Advocate for our patients • It’s the right thing to do • Makes good business sense (did I say that) • Will force the payments to align to the services and procedures • Will correct the political climate Neltner Billing & Consulting Services
Agenda • The Solutions • Patient care – the first solution • Relative Value Units (and cost) – the second solution • E&M coding – the third solution • Prolonged services – the fourth solution • How clinical documentation can tell the story of complexity • Drugs – the fifth solution • CMS strategy – Newt Gringrich Connection • Pay-for Performance • A new solution for oncology • How to get paid for generating the data? • How oncology can partner with CMS to offer “Value Based Purchasing” Neltner Billing & Consulting Services
Patients First • Who speaks for our patients? • Are patients aware of our costs? • Do patient understand our costs? • Let the buyer beware • What is best for our patients when it comes to our involvement in the drugs? • I would love to tell a patient “we have no financial interest in the drugs” • I would love to tell a patient “I don’t do the lunch and I don’t take the gifts” Neltner Billing & Consulting Services
RVUs Second • SOAC - NEW WORD ON THE BLOCK • Our basis for payment is our complex cognitive resource that is under the microscope and not on the table for full viewing. • We need to generate the data under appropriate leadership that can prove • PHYSICIAN WORK • PRACTICE EXPENSE • DATA SHOULD SHOW SAVINGS TO HEALTH PLANS • THE PEN IS THE PHYSICIAN’S WEAPON Neltner Billing & Consulting Services
E&M Coding Third • We can begin the process to bill appropriately • “FAILURE IS NOT AN OPTION” • THERE ARE EFFICIENT, EASY TOOLS TO ACCOMPLISH THIS TASK Neltner Billing & Consulting Services
Prolonged Services Fourth • How clinical documentation can tell the story of complexity • INSTILL THE PROCESS • PROLONGED IS NOT CONTINUOUS • DEAL WITH FACE-TO-FACE • RVU SAYS ITS CLINICAL TIME • EDUCATE EVERYONE • BEGIN BILLING • BEGIN THE DEBATE • BE PREPARED TO GO THE EXTRA MILE • THAT IS WHAT THE ALJ PROCESS IS ALL ABOUT Neltner Billing & Consulting Services
Drugs Fifth • STOP THE LUNCHES AND FREE GIFTS • EMBRACE THE STRATEGY • TELL CONGRESS THEY DON’T NEED ASP • THEY NEED A PARTNER: US • THE HEALTH CARE COMMUNITY NEEDS LPC “LOWEST POSSIBLE COST” Neltner Billing & Consulting Services